Last reviewed: March 2026Contents
MDM Templates
Paroxysmal / New-Onset AFib
Patient with new-onset / paroxysmal atrial fibrillation presenting with palpitations. Hemodynamically stable with no signs of acute decompensation. No chest pain, no dyspnea at rest, no syncope, no acute heart failure. Tolerating PO.
History and exam lower suspicion for precipitating causes including ACS, pulmonary embolism, pneumothorax, tamponade, thyrotoxicosis, sepsis, and decompensated heart failure.
CHA₂DS₂-VASc score: ***.
HAS-BLED score: ***.
Spontaneously converts to NSR during observation:
Plan: Initiate anticoagulation per CHA₂DS₂-VASc (see below). Start rate control with metoprolol 25mg PO BID. Cardiology referral for new diagnosis.
Disposition: Discharge after sustained NSR on monitor. PCP follow-up within 48 hours. Return for recurrent palpitations, chest pain, syncope, or dyspnea.
Remains in AFib, rate controlled, hemodynamically stable:
Plan: Rate control achieved with HR <110 (per RACE-II target).[1] Initiate anticoagulation per CHA₂DS₂-VASc. Start oral rate control agent.
Disposition: Discharge with cardiology follow-up within 1 week for rhythm vs rate control strategy discussion. / Admit for observation if symptomatic or rate refractory.
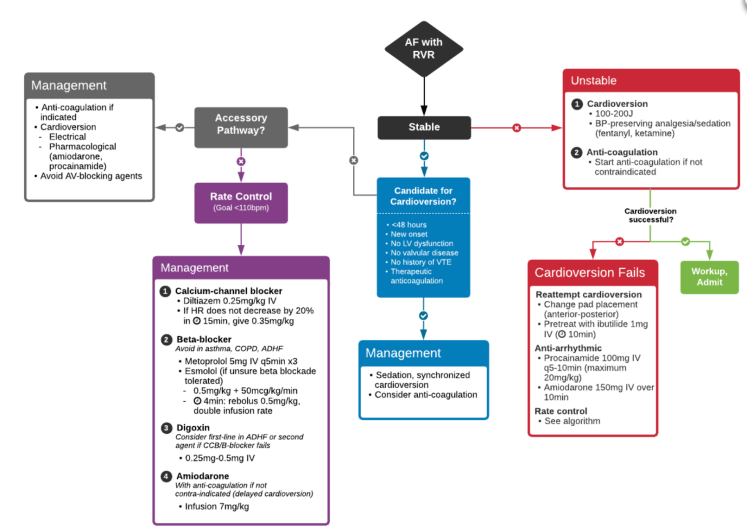
AFib with RVR
Patient presenting in atrial fibrillation with rapid ventricular response requiring immediate rate control. Exam reassuring for medication based treatment: No hypotension, no AMS, no acute heart failure, no signs of end-organ hypoperfusion.
History and exam lower suspicion for precipitating causes including ACS, PE, pneumothorax, tamponade, thyrotoxicosis, sepsis, and decompensated heart failure. ECG without pre-excitation pattern (ruling out WPW — see below).
Stable, no heart failure:
Plan: IV diltiazem 0.25mg/kg (typically 15-20mg) over 2 min. If inadequate response at 15 min, repeat 0.35mg/kg (typically 20-25mg). If responds — start diltiazem infusion 5-15mg/hr or transition to PO diltiazem 30-60mg q6h.[2]
Alternative: Metoprolol 5mg IV q5min x 3 doses, then oral metoprolol 25-50mg if responds.
Target: HR <110 per RACE-II.[1]
Unstable (hypotension, AMS, acute HF, chest pain with ischemia):
Plan: Synchronized cardioversion at 200J biphasic. See procedure note and cardioversion pearls below.
Disposition: Admit.
Admit if: Refractory RVR despite IV rate control, new-onset with hemodynamic compromise, concern for precipitating cause requiring inpatient workup, or concurrent acute HF.
Procedure Notes
Synchronized Cardioversion
Indication: Atrial fibrillation/flutter with hemodynamic instability / elective cardioversion within 48h of onset / TEE-confirmed no LAA thrombus
Time Out: Correct patient, correct procedure confirmed
Sedation: Etomidate *** mg IV + ketamine *** mg IV (analgesic dose). BVM and suction at bedside. Continuous monitoring.
Safety Check: Defibrillator in SYNC mode confirmed — sync markers visible on R waves on monitor
Methods: Anterior-posterior pad placement. Synchronized cardioversion delivered at 200J biphasic. / Repeat at ***J.
Result: Successful conversion to normal sinus rhythm confirmed on 12-lead ECG post-procedure. / Unsuccessful — remained in AFib.
Complications: None. Patient tolerated procedure well. Recovered from sedation without incident.
Clinical Education
Rate Control Agents
| Agent | IV Dose | Oral Transition | Pearl |
| Diltiazem | 0.25mg/kg IV, repeat 0.35mg/kg at 15min | 30-60mg PO q6h or 120-360mg ER daily | Fastest onset. Avoid in HFrEF (negative inotropy)[2] |
| Metoprolol | 5mg IV q5min x 3 doses | 25-50mg PO BID (or succinate 50-200mg daily) | Safe in HF (already on it). Slower onset than diltiazem |
| Amiodarone | 150mg IV over 10min, then 1mg/min x 6h | 200mg PO BID-TID (loading) | Rate AND rhythm control. Use for AFib + HF. Drip = significant volume[3] |
| Digoxin | 0.25mg IV, repeat q2h (max 1.5mg/24h) | 0.125-0.25mg PO daily | Slow onset (2-6h). Adjunct in HF when BB/CCB insufficient. Narrow TI |
| Magnesium | 2g IV over 15min | — | Adjunct — assists rate control, may help conversion. Replete regardless[4] |
RACE-II target: HR <110 at rest is non-inferior to strict control (<80). Avoid chasing a normal heart rate — it’s more important that the patient is asymptomatic and hemodynamically stable.[1]
Cardioversion Pearls
The 48-hour rule: If AFib onset is clearly <48 hours, cardioversion can be performed without prior anticoagulation or TEE. If onset is >48 hours or uncertain, the patient needs either 3 weeks of therapeutic anticoagulation prior to cardioversion or a TEE to rule out LAA thrombus before proceeding.[5]
Don’t pretreat with rate control before cardioversion. IV rate/rhythm control agents given before cardioversion reduce its effectiveness — 90% success first-line drops to ~60% after pretreatment. If the decision is to cardiovert, just cardiovert.[6]
Energy: Start at 200J biphasic (or 150J for some devices). Anterior-posterior pad placement is more effective than anterior-lateral. Make sure SYNC mode is confirmed — look for sync markers on R waves before firing.[5]
Sedation: Ottawa Aggressive Protocol uses etomidate 5-7mg IV + analgesic-dose ketamine 10-15mg IV. Propofol 0.5-1mg/kg IV is an alternative. Have BVM, suction, and airway equipment at bedside. Push-dose epi drawn up for post-cardioversion hypotension.
Post-cardioversion: 12-lead ECG to confirm NSR. Anticoagulation for minimum 4 weeks after cardioversion regardless of CHA₂DS₂-VASc (atrial stunning). Longer-term anticoagulation decision per CHA₂DS₂-VASc.[5]
Anticoagulation & CHA₂DS₂-VASc
DOACs are first-line over warfarin for non-valvular AFib per 2023 ACC/AHA/ACEP guidelines. Aspirin is no longer recommended for stroke prevention in AFib — it provides minimal benefit with meaningful bleeding risk.[7]
| CHA₂DS₂-VASc | Recommendation |
| 0 (male) or 1 (female) | No anticoagulation |
| 1 (male) | Consider anticoagulation — discuss risk/benefit |
| ≥2 | Anticoagulation recommended[7] |
| DOAC | Standard Dose | Dose Reduction |
| Apixaban (Eliquis) | 5mg PO BID | 2.5mg BID if ≥2 of: age ≥80, weight ≤60kg, Cr ≥1.5 |
| Rivaroxaban (Xarelto) | 20mg PO daily with food | 15mg daily if CrCl 15-50 |
| Dabigatran (Pradaxa) | 150mg PO BID | 75mg BID if CrCl 15-30 |
| Edoxaban (Savaysa) | 60mg PO daily | 30mg daily if CrCl 15-50 or weight ≤60kg |
Pearl: Use HAS-BLED to assess bleeding risk — a high score doesn’t mean “don’t anticoagulate,” it means optimize modifiable risk factors (HTN control, stop unnecessary NSAIDs/antiplatelet agents, reduce alcohol). Most patients with high CHA₂DS₂-VASc benefit from anticoagulation even with elevated HAS-BLED.[7]
AFib with Heart Failure
Avoid diltiazem and verapamil in HFrEF — negative inotropy can precipitate decompensation. Beta-blockers should also be used cautiously in acute decompensated HF.[3]
| HF Severity | Rate Control Strategy |
| Mild HF (warm, non-hypotensive) | Low-dose diltiazem 10mg IV + furosemide 40mg IV (or double home dose). Transition to PO diltiazem 30mg q6h if responds. Treat the HF simultaneously. |
| Moderate-Severe HF (hypotensive, pulmonary edema) | Amiodarone 150mg IV over 10min then 1mg/min (rate + rhythm control, safe in HF). Digoxin 0.25mg IV q2h as adjunct (slow onset 2-6h). Avoid BB and CCB.[3] |
Pearl: Amiodarone drip runs at ~33mL/hr — that’s almost 800mL over 24 hours. In a patient with decompensated HF, that volume matters. If running a long drip, account for it in your fluid balance and adjust diuretics accordingly.
AFib with WPW
This is the AFib that kills. AFib conducting down an accessory pathway bypasses the AV node’s rate-limiting function — ventricular rates can exceed 250-300bpm and degenerate into VFib.[8]
Recognize it: Irregularly irregular wide-complex tachycardia with varying QRS morphology and very fast rates. If you see AFib with a wide QRS and rate >200, think WPW until proven otherwise.
Do NOT give AV nodal blockers — diltiazem, beta-blockers, digoxin, and adenosine are all contraindicated. They block the AV node and force more conduction down the accessory pathway, potentially causing VFib and arrest.[8]
Treatment: If unstable — immediate synchronized cardioversion at 200J. If stable — procainamide 15-18mg/kg IV over 30-60min (slows accessory pathway conduction). Have the defibrillator pads on and ready to shock.
ED Workup
Every new AFib gets: 12-lead ECG (confirm rhythm, rule out pre-excitation, assess for ischemia), troponin (ACS as precipitant), BNP (HF), TSH (thyrotoxicosis), BMP (electrolytes), Mg level, CBC, CXR (HF, PNA, PTX).
Don’t forget reversible causes: The AF onset may be the symptom, not the disease. Always consider PE (tachycardia, hypoxia, risk factors), sepsis (fever, WBC), thyrotoxicosis (tremor, weight loss, warm skin), alcohol/stimulant use, and postoperative state.
References
- Van Gelder IC et al. Lenient versus Strict Rate Control in Patients with Atrial Fibrillation (RACE II). NEJM. 2010;362(15):1363-1373. PubMed
- Fromm C et al. Diltiazem vs. Metoprolol in the Management of Atrial Fibrillation or Flutter with Rapid Ventricular Rate in the Emergency Department. J Emerg Med. 2015;49(2):175-182. PubMed
- Joglar JA et al. 2023 ACC/AHA/ACEP/HRS Guideline for Diagnosis and Management of Atrial Fibrillation. Circulation. 2024;149(1):e1-e156. PubMed
- Bouida W et al. Low-Dose Magnesium Sulfate versus High-Dose in the Early Management of Rapid Atrial Fibrillation. Acad Emerg Med. 2019;26(2):183-191. PubMed
- January CT et al. 2019 AHA/ACC/HRS Focused Update of the 2014 Guideline for Management of Patients with Atrial Fibrillation. Circulation. 2019;140(2):e125-e151. PubMed
- Blecher GE et al. ED Management of Acute Atrial Fibrillation: Does Pre-treatment with Rate/Rhythm Control Agents Reduce Cardioversion Success? Emerg Med Australas. 2012;24(5):508-514. PubMed
- Joglar JA et al. 2023 ACC/AHA/ACEP/HRS Guideline for Diagnosis and Management of Atrial Fibrillation: Anticoagulation Recommendations. J Am Coll Cardiol. 2024;83(1):109-279. PubMed
- Brugada J et al. 2019 ESC Guidelines for the Management of Patients with Supraventricular Tachycardia. Eur Heart J. 2020;41(5):655-720. PubMed
