Last reviewed: March 2026
Contents
MDM Templates
BPPV
Patient presents with episodic positional vertigo lasting seconds, provoked by head movement. No hearing loss, no headache, no focal neurologic deficits. Dix-Hallpike positive with fatigable upbeating torsional nystagmus.
Presentation classic for BPPV. Not consistent with stroke (episodic, positional, fatigable nystagmus, no focal deficits), vestibular neuritis (no persistent vertigo between episodes), or Meniere disease (no hearing loss, no tinnitus, no aural fullness).
Plan: Epley maneuver performed with resolution of symptoms. Discharge with return precautions for persistent vertigo, new headache, focal weakness, or difficulty speaking.
Vestibular Neuritis / Labyrinthitis
Patient presents with acute onset continuous vertigo, nausea, and gait unsteadiness. No hearing loss, no focal neurologic deficits. Nystagmus is unidirectional and horizontal, suppressed by visual fixation.
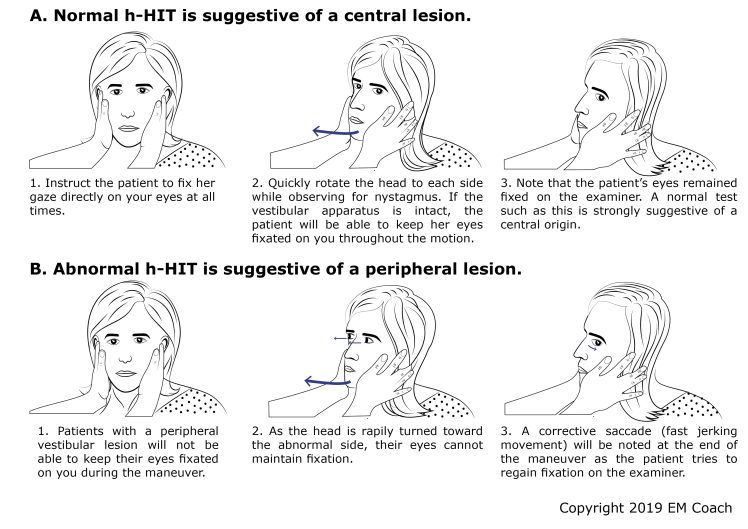
Presentation consistent with vestibular neuritis. HINTS exam reassuring — head impulse test abnormal (corrective saccade present), nystagmus unidirectional, no skew deviation. Not consistent with posterior circulation stroke (HINTS peripheral pattern, no focal deficits), BPPV (continuous, not episodic), or CNS infection (afebrile, no meningismus).
If hearing loss present: Labyrinthitis rather than isolated vestibular neuritis. Same management but warrants ENT follow-up for audiometry.
Plan: Symptomatic treatment with meclizine and ondansetron. Discharge with PCP follow-up. Return for worsening symptoms, new headache, focal weakness, or difficulty speaking.
Central Vertigo / Posterior Circulation Concern
Patient presents with acute vertigo and exam findings concerning for central cause. HINTS exam concerning — normal head impulse test (no corrective saccade), direction-changing nystagmus, or skew deviation present.
Any one of these HINTS findings raises concern for posterior circulation stroke. Not consistent with peripheral vestibular cause given central HINTS pattern. Additional concerning features include severe gait ataxia out of proportion to vertigo, new headache, or other focal neurologic deficits.
If neurology consulted: Neurology consulted regarding patient’s exam findings, imaging, and disposition.
Plan: MRI brain with diffusion-weighted imaging. Admit for stroke workup.
Clinical Education
Approach to Dizziness
Stop asking “is it vertigo, presyncope, or disequilibrium?” This traditional approach has been shown to be unreliable — patients reclassify their symptoms up to 50% of the time when asked again. Instead, classify by timing and triggers: episodic vs continuous, spontaneous vs positional, and with or without neurologic symptoms.[1]
The dangerous diagnosis is posterior circulation stroke. Cerebellar and brainstem strokes present with vertigo, nausea, and gait unsteadiness — identical to vestibular neuritis. CT is useless for posterior fossa strokes (misses up to 40%). MRI with DWI is the imaging of choice, but even MRI can miss posterior strokes in the first 24–48 hours. The bedside HINTS exam outperforms early MRI for identifying stroke in acute vestibular syndrome.[2]
The HINTS Exam
HINTS is only valid in acute vestibular syndrome — acute onset continuous vertigo with nystagmus. It is not useful for episodic dizziness, presyncope, or the patient who is no longer symptomatic. All three components must be performed:
| Test | Peripheral (Reassuring) | Central (Dangerous) |
| Head Impulse | Abnormal (corrective saccade present) | Normal (no corrective saccade) |
| Nystagmus | Unidirectional, horizontal | Direction-changing or purely vertical/torsional |
| Test of Skew | Absent (no skew deviation) | Present (vertical misalignment on alternate cover test) |
A negative HINTS exam (all three peripheral) rules out stroke better than a negative MRI with DWI in the first 24–48 hours — sensitivity >96% vs ~80% for early MRI. Any single dangerous finding on HINTS should prompt stroke workup.[2]
Central vs Peripheral Vertigo
| Feature | Peripheral | Central |
| Onset | Sudden | Gradual or sudden |
| Nystagmus | Unidirectional, suppressed by fixation | Direction-changing, not suppressed |
| Hearing loss | May be present (labyrinthitis, Meniere) | Rare (AICA stroke can cause it) |
| Gait | Unsteady but can walk | Severely ataxic, may not be able to sit |
| Focal deficits | Absent | May be present (diplopia, dysarthria, Horner) |
Caveat: AICA stroke can mimic peripheral vertigo — it can cause hearing loss and an abnormal head impulse test because AICA supplies the labyrinth. If the patient has hearing loss with vertigo and any other red flags, get the MRI regardless of HINTS findings.[3]
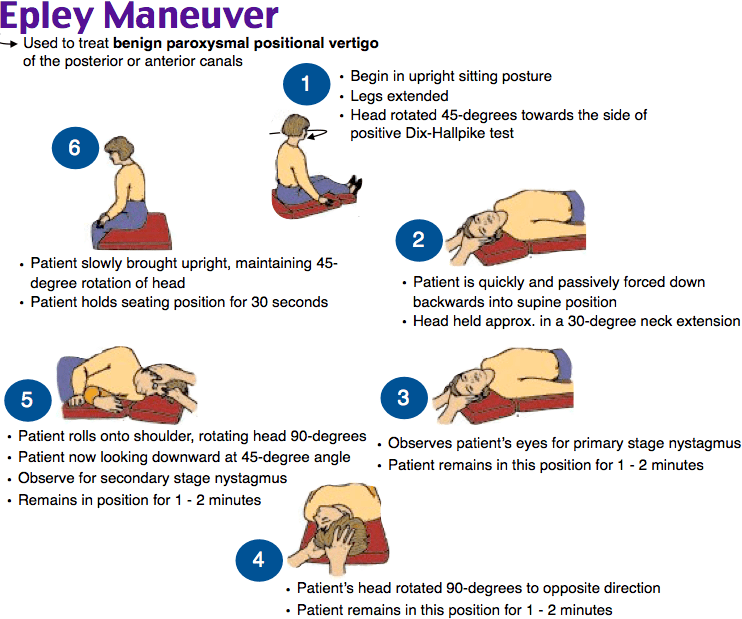
BPPV and the Epley
Dix-Hallpike is diagnostic. Positive when the patient develops upbeating, torsional nystagmus after a latency of 1–5 seconds, lasting <60 seconds, and fatiguing with repeat testing. The affected ear is the one that is down when nystagmus is provoked. Downbeating nystagmus on Dix-Hallpike is NOT BPPV — it suggests a central cause.
The Epley maneuver is the treatment and works immediately in ~80% of cases. No medications needed. Meclizine is a vestibular suppressant that masks symptoms without treating the cause — use only as a bridge if the Epley doesn’t fully resolve symptoms.[4]
Peripheral Vestibular Causes
| Diagnosis | Key Features | Treatment |
| BPPV | Episodic, seconds, positional, Dix-Hallpike positive | Epley maneuver |
| Vestibular neuritis | Continuous vertigo, days, no hearing loss | Supportive, meclizine, ondansetron |
| Labyrinthitis | Vestibular neuritis + hearing loss | Same as neuritis + ENT follow-up |
| Meniere disease | Episodic vertigo + hearing loss + tinnitus + aural fullness | Meclizine, low-salt diet, ENT follow-up |
| Acoustic neuroma | Gradual unilateral hearing loss + tinnitus | MRI, ENT/neurosurgery referral |
Disposition
Discharge: BPPV (after successful Epley), vestibular neuritis/labyrinthitis with reassuring HINTS exam, Meniere disease with controlled symptoms. All with PCP or ENT follow-up.
Admit: Any concern for central cause (abnormal HINTS, focal deficits, severe ataxia), intractable vomiting with inability to tolerate oral medications, or significant fall risk in an elderly or debilitated patient.
Don’t send patients home unable to walk. Even if you’re confident in a peripheral diagnosis, a patient with severe unsteadiness needs to be able to safely ambulate or have reliable support at home before discharge.
References
- Newman-Toker DE, Edlow JA. TiTrATE: a novel, evidence-based approach to diagnosing acute dizziness and vertigo. Neurol Clin. 2015;33(3):577-599. PubMed
- Kattah JC, Talkad AV, Wang DZ, et al. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009;40(11):3504-3510. PubMed
- Lee H, Kim JS, Chung EJ, et al. Infarction in the territory of anterior inferior cerebellar artery: spectrum of audiovestibular loss. Stroke. 2009;40(12):3745-3751. PubMed
- Hilton MP, Pinder DK. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database Syst Rev. 2014;(12):CD003162. PubMed
