Last reviewed: March 2026
Contents
MDM Templates
Mild / Moderate MVA — Discharge
Patient presents after motor vehicle collision complaining of pain to ***. They are hemodynamically stable with a non-focal neurological exam, alert and not intoxicated, without distracting injury. No recurrent vomiting and no signs of basilar skull fracture.
Given history, exam, and workup, low suspicion for intracranial hemorrhage, skull fracture, cervical spine fracture or acute spinal syndrome, pneumothorax, pulmonary contusion, cardiac contusion, aortic or vertebral dissection, hollow organ injury, acute traumatic abdomen, significant hemorrhage, or extremity fracture.
C-spine imaging deferred — no midline tenderness, moves neck freely, no bony step-offs, negative by NEXUS criteria. FAST deferred — hemodynamically stable, no abdominal tenderness, no external signs of torso trauma, low-energy mechanism. Stable gait and tolerating PO.
Plan: Analgesics.
Disposition: Discharge with strict return precautions. Patient counseled that some injuries (such as delayed duodenal injury) may present in a delayed fashion. Follow up with PCP within 48 hours.
If managed as trauma activation:
Patient managed in conjunction with the trauma surgeon as a trauma activation. The trauma surgeon has determined that the patient is safe for discharge.
Trauma Activation
Patient presents after high-energy mechanism as a trauma activation. Managed in conjunction with trauma surgery. ATLS primary and secondary survey completed.
Trauma surgery team directing workup, imaging, and disposition.
Plan: Resuscitation per ATLS protocol. Pan-scan imaging per institutional protocol.
Disposition: Per trauma surgery.
Clinical Education
Reassuring Exam Factors
The clinical exam is the most powerful tool in minor trauma disposition. A patient who is hemodynamically stable, has a non-focal neuro exam, is alert with no distracting injury, moves their neck freely without midline tenderness, has a non-tender abdomen without bruising, and is ambulatory with stable gait — this patient very likely does not have a clinically significant injury. The exam findings that matter most: midline cervical tenderness (c-spine fracture), abdominal tenderness or seatbelt sign (intra-abdominal injury), focal neuro deficit (intracranial or cord injury), and chest wall instability (rib fractures, flail segment).[1]
C-Spine Injury Pearls
Stable cervical fractures can go home with a collar. Isolated spinous process fractures (Clay Shoveler’s), isolated transverse process fractures (without transverse foramen involvement), and Type I odontoid fractures (avulsion without atlantooccipital dislocation) are mechanically stable. Discharge in a cervical collar with neurosurgery follow-up in 1–2 weeks for flexion-extension views or MRI.[2]
Transverse process fractures involving the transverse foramen may indicate vertebral artery injury — get a CTA neck and spine consultation.
Burst fractures of the vertebral body: stable if no anterior cord syndrome symptoms (check motor and pain/temperature sensation). If the patient has neurological deficits suggesting cord compression from retropulsed fragments, this is a surgical emergency.
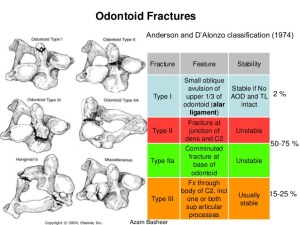
Odontoid fracture classification — AOD = atlanto-occipital dislocation
Spinal Cord Syndromes
Anterior cord syndrome has the worst prognosis — most patients do not regain motor function. This affects the corticospinal (motor) and spinothalamic (pain/temperature) tracts while sparing the dorsal columns (proprioception, vibration). Typically caused by flexion injuries or vascular compromise to the anterior spinal artery.[3]
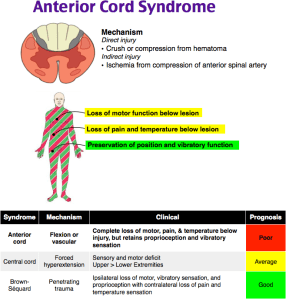
Anterior cord syndrome — motor loss and pain/temperature loss with preserved proprioception
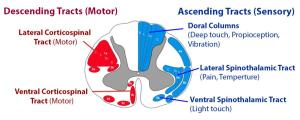
Spinal cord pathways
Central cord syndrome — upper extremity weakness greater than lower extremity weakness. Most common in elderly with pre-existing cervical spondylosis after a hyperextension injury. Better prognosis — many recover significant function.
Brown-Séquard syndrome — hemisection of the cord. Ipsilateral motor loss and proprioception loss, contralateral pain/temperature loss. Best prognosis of the incomplete cord syndromes.
Splenic Laceration Pearls
Not every splenic laceration goes to the OR. Non-operative management is now standard for hemodynamically stable patients with grades I–III injuries. Indications for surgery: hemodynamic instability, generalized peritonitis, altered mental status (can’t serially exam), grade IV or higher, and >4 units PRBC transfused. Age >55 carries higher risk of failure of non-operative management — lower your threshold for surgery or angioembolization in this group.[4]
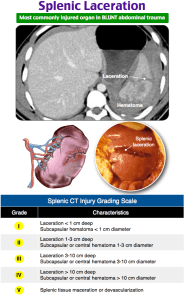
Splenic injury grading
Hemorrhagic Shock Classification
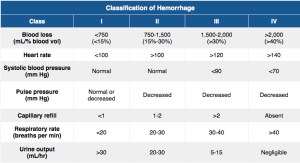
ATLS Classification of Hemorrhagic Shock
Class I (up to 750 mL) and Class II (750–1500 mL) may have minimal vital sign changes. Don’t be falsely reassured by normal vitals in a young trauma patient — they compensate until they crash. Tachycardia is often the first sign. A narrowing pulse pressure (rising diastolic) precedes frank hypotension. Base deficit and lactate are more sensitive markers of occult hemorrhage than vitals alone.[5]
Neurogenic vs Spinal Shock
| Feature | Neurogenic Shock | Spinal Shock |
| Mechanism | Loss of sympathetic tone | Temporary loss of all cord function below injury |
| Hemodynamics | Hypotension + bradycardia | Normal |
| Neuro exam | Deficit consistent with cord level | Areflexia and flaccid paralysis |
| Key point | Treat as hemorrhagic shock until proven otherwise in trauma | Temporary — reflexes return |
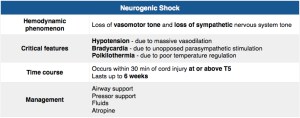
Critical point: In a trauma patient, neurogenic shock is a diagnosis of exclusion. Assume hemorrhagic shock until you’ve ruled it out — don’t let warm dry skin and bradycardia lull you into skipping the FAST and CXR.
Delayed Injury Presentations
Counsel every discharged trauma patient about delayed injury. Duodenal hematoma/perforation can present days after blunt abdominal trauma. Splenic rupture can have a “two-hit” presentation — initial subcapsular hematoma that ruptures later. Epidural hematomas famously have a “lucid interval.” Include specific return precautions for abdominal pain, worsening headache, new neurological symptoms, and chest pain.[6]
Pelvic fractures in blunt trauma with hemodynamic instability carry ~50% mortality — this is a resuscitation emergency requiring pelvic binder, massive transfusion, and early angioembolization or operative hemorrhage control.
References
- Stiell IG et al. The Canadian CT head rule for patients with minor head injury. Lancet. 2001;357(9266):1391-1396. PubMed
- Goldberg W et al. Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med. 2001;38(1):17-21. PubMed
- McKinley W et al. Incidence and outcomes of spinal cord injury clinical syndromes. J Spinal Cord Med. 2007;30(3):215-224. PubMed
- Stassen NA et al. Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S294-S300. PubMed
- ATLS Subcommittee. Advanced Trauma Life Support. 10th ed. American College of Surgeons. 2018.
- Nance ML, Nance FC. Delayed presentation of splenic injury. Surgery. 1996;119(5):588-590.
