Last reviewed: March 2026Contents
MDM Templates
Sore Throat NOS
No history of immunocompromised state.
Nontoxic appearance. No trismus.
No airway compromise. Able to tolerate PO.
Given History and Exam I have low suspicion for this presentation being caused by PTA, RPA, Ludwig’s, Epiglottitis, Bacterial Tracheitis, acute HIV, or Strep throat.
Rx: Conservative care
Disposition: Discharge home with prompt outpatient PCP follow up; return precautions discussed. Return for worsening pain, inability to swallow, drooling, voice changes, difficulty breathing, or fever.
Peritonsillar Abscess (PTA)
Presentation most consistent with RIGHT/LEFT sided Peritonsillar Abscess. Normal vitals, well appearing, normal neck ROM, tolerating secretions, and protecting airway. Given History and Exam I have a lower suspicion for RPA, Ludwig’s, epiglottitis, acute HIV, Strep, or EBV.
Interventions:
- Needle aspiration of abscess
- Methylprednisolone 125mg IV or Dexamethasone 10mg IV/IM
- Pain control
Rx: Clindamycin 300mg PO Q6hrs x 10 days (or Augmentin 875/125 PO BID x 10 days)
Disposition: Discharge with instructions for prompt ENT and primary care follow-up. Return for worsening swelling, inability to swallow, difficulty breathing, or recurrent fever.
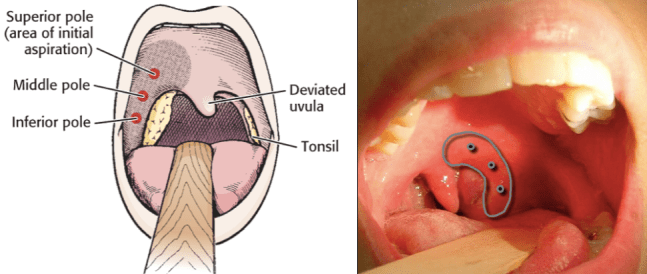
PTA Aspiration Procedure Note:
Location: The patient’s RIGHT/LEFT peritonsillar region was addressed.
Time out: A time out was undertaken to determine that this was the correct patient and the correct procedure.
Methods: Topical analgesic spray was used to anesthetize the oropharynx. An 18-gauge needle was inserted into the peritonsillar tissue and approximately ___ mLs of purulent material was drained.
Safety Check: The patient tolerated this procedure well and there were no complications.
Retropharyngeal Abscess (RPA)
Patient presenting with worsening sore throat with exam and imaging consistent with retropharyngeal abscess.
No trismus, euvolemic, no airway compromise.
Interventions:
- CT neck with IV contrast obtained
- IV antibiotics: Unasyn (ampicillin/sulbactam) 3g IV OR Clindamycin 900mg IV
- IVF resuscitation
- ENT consultation for operative drainage vs trial of IV antibiotics
Disposition: Admit. ENT consulted for evaluation for operative drainage. If small/early abscess, may trial IV antibiotics with close monitoring per ENT recommendation.
Epiglottitis
Patient presenting with acute onset sore throat, odynophagia, and *muffled voice / stridor / drooling*. Exam and imaging concerning for epiglottitis.
Interventions:
- Maintain calm, upright positioning — avoid agitating patient
- Nebulized racemic epinephrine if stridor
- IV antibiotics: Ceftriaxone 2g IV + Dexamethasone 10mg IV
- Difficult airway equipment at bedside. Anesthesia and/or ENT at bedside for airway management.
Disposition: Admit to ICU. Airway intervention if worsening. ENT consulted.
Clinical Education
The Dangerous Sore Throat — Don’t-Miss Diagnoses
Most sore throats are viral and benign. The job in the ED is to identify the ones that can kill — usually by airway compromise or sepsis. Key red flags on any sore throat presentation:
- Trismus (inability to fully open mouth) — PTA until proven otherwise
- “Hot potato” / muffled voice — PTA, RPA, or supraglottic pathology
- Drooling / inability to swallow secretions — epiglottitis, severe PTA, Ludwig’s
- Stridor — impending airway compromise, epiglottitis, RPA, angioedema
- Neck swelling / floor-of-mouth elevation — Ludwig’s angina
- Uvular deviation — PTA (deviates AWAY from abscess)
- Rigors + sore throat + neck pain along SCM — Lemierre syndrome
- Recent dental procedure / dental pain + submandibular swelling — Ludwig’s
Peritonsillar Abscess (PTA) Pearls
Diagnosis: Clinical diagnosis. CT is NOT required if presentation is classic (trismus, uvular deviation, unilateral tonsillar swelling/fullness, muffled voice). CT neck with IV contrast is helpful when RPA or other deep space infection is on the differential, or if the exam is equivocal.[1]
Intraoral ultrasound can differentiate abscess from phlegmon/cellulitis and guide aspiration. Sensitivity ~90% for identifying drainable fluid collection.[2] Useful when exam is uncertain or to confirm needle target.
Aspiration vs I&D: Needle aspiration is first-line in the ED — equivalent success rate to I&D with less pain and no need for ENT in most cases.[3] Recurrence rate after aspiration ~10–15%. If aspiration is dry (no pus), consider phlegmon → trial of IV antibiotics and steroids.
Steroids: Single-dose IV dexamethasone (10mg) or methylprednisolone (125mg) reduces pain, trismus, and time to oral intake. Evidence supports routine use.[4]
Antibiotics:
- Outpatient: Clindamycin 300mg PO QID x 10d OR Augmentin 875/125 PO BID x 10d
- Inpatient/IV: Unasyn 3g IV q6h OR Clindamycin 900mg IV q8h
- Must cover Group A Strep AND oral anaerobes (Fusobacterium, Prevotella)
Disposition pearl: Most PTAs can be drained and discharged if the patient can tolerate PO, has no airway concern, and has reliable follow-up. Admit if: unable to tolerate PO post-drainage, immunocompromised, concern for deep space extension, or failed outpatient therapy.
Retropharyngeal Abscess (RPA) Pearls
Two populations: Children <5 years (suppurative lymph nodes from URI/pharyngitis — retropharyngeal lymph nodes involute by ~age 5) and adults (usually from penetrating trauma, dental infection, or instrumentation).[5]
Classic presentation: Fever, neck stiffness/pain (especially with extension), dysphagia, drooling, muffled voice. Children may present with neck held in extension, refusal to eat, and irritability. Adults may present more indolently.
Imaging: CT neck with IV contrast is the study of choice. Look for hypodense fluid collection in the retropharyngeal space with rim enhancement. Lateral neck XR can be a screening tool in peds — retropharyngeal soft tissue >7mm at C2 or >14mm at C6 (adult: >22mm at C6) suggests pathology, but sensitivity is limited.[5]
See: Radiopaedia — Retropharyngeal Abscess CT examples
Danger: Retropharyngeal space communicates with the mediastinum (“danger space”). Extension → mediastinitis, which carries >40% mortality. Airway compromise, internal jugular thrombosis, and carotid erosion are also life-threatening complications.[6]
Management: ENT consult for drainage (operative) vs trial of IV antibiotics for small/early abscess or phlegmon. Abx: Unasyn 3g IV q6h or Clindamycin 900mg IV q8h. Always admit.
Ludwig’s Angina
What it is: Bilateral infection of the submandibular, sublingual, and submental spaces — typically from dental infection (2nd/3rd molars). Rapidly progressive cellulitis, NOT a true abscess (no drainable collection early on).[7]
Classic presentation: “Bull neck” — bilateral submandibular swelling, floor-of-mouth elevation (“woody” induration), tongue protrusion/displacement posteriorly, drooling, trismus, dysphagia. Fever.
Why it kills: Posterior tongue displacement → airway obstruction. This is an airway emergency first, infection second.
Airway management: Fiberoptic nasotracheal intubation is preferred. Awake intubation with sedation. Have surgical airway (cricothyrotomy) ready. Do NOT paralyze — loss of muscle tone worsens obstruction. Avoid blind oral intubation.[7]
See: Radiopaedia — Ludwig’s Angina CT and clinical images
Antibiotics: Unasyn (ampicillin/sulbactam) 3g IV q6h OR Penicillin G + Metronidazole. Clindamycin 900mg IV q8h if PCN allergy. Must cover strep and oral anaerobes.
Disposition: Always admit. ENT and/or OMFS consult. ICU if any airway concern.
Epiglottitis Pearls
Epidemiology shift: Since the Hib vaccine, epiglottitis is now predominantly an adult disease. Adult epiglottitis is more indolent than pediatric but still carries significant airway risk.[8]
Classic presentation: Acute severe sore throat with odynophagia disproportionate to exam findings, muffled voice, drooling, “tripod” positioning. Exam may show a relatively benign-appearing oropharynx — the pathology is supraglottic and not visible on routine exam.
Imaging: Lateral neck XR shows “thumbprint sign” (swollen epiglottis). CT neck with IV contrast provides better detail. In a stable patient, imaging before laryngoscopy is reasonable. In an unstable patient, go directly to the OR/airway management.
See: Radiopaedia — Epiglottitis: thumbprint sign and CT examples
Key pearl: Sore throat with “pain out of proportion to exam” + drooling or voice change = epiglottitis until proven otherwise. The oropharynx can look deceptively normal.
Management:
- Keep patient calm and upright — agitation worsens airway obstruction
- Nebulized racemic epinephrine for stridor
- Dexamethasone 10mg IV (reduces edema)
- Ceftriaxone 2g IV (cover H. influenzae, Strep, Staph)[8]
- Difficult airway equipment at bedside; anesthesia/ENT for airway management
- Avoid blind nasopharyngeal suctioning or tongue depressor exam in children with suspected epiglottitis — can trigger complete obstruction
Lemierre Syndrome
What it is: Septic thrombophlebitis of the internal jugular vein, almost always caused by Fusobacterium necrophorum, typically following pharyngitis or PTA in young, healthy adults.[9]
Classic presentation: Young adult with recent pharyngitis (often 1–2 weeks prior) who develops rigors, high fevers, and neck pain/swelling along the SCM. Septic emboli to lungs (cavitary lesions, empyema), joints, liver, and brain can follow.
Why it’s missed: Often dismissed as “post-viral illness” or “persistent pharyngitis.” The sore throat may have resolved by the time septic complications appear. Think of it when a young patient with recent pharyngitis develops unexplained sepsis or pulmonary nodules/cavitations on CXR or CT chest.[9]
Imaging: CT neck with IV contrast — look for thrombus in the internal jugular vein with surrounding fat stranding. CT chest may show septic pulmonary emboli (peripheral cavitary nodules).
See: Radiopaedia — Lemierre Syndrome imaging examples
Treatment: Prolonged IV antibiotics (metronidazole + beta-lactam, or monotherapy with Unasyn or meropenem). Duration typically 4–6 weeks. Anticoagulation is controversial — no RCT evidence, but often used if thrombus is extensive or propagating.[9]
Strep Pharyngitis & Centor Score
When to test: Use the Modified Centor (McIsaac) Score to guide testing. Score 0–1: no testing needed, viral likely. Score 2–3: rapid strep test. Score 4+: empiric treatment reasonable, though most guidelines still recommend test confirmation.[10]
Treatment:
- Adults: Penicillin V 500mg PO BID x 10 days OR Amoxicillin 1g PO daily x 10 days
- Pediatric: Amoxicillin 50mg/kg/day (max 1g) PO daily x 10 days OR Penicillin V 250mg PO BID x 10 days
- PCN allergy: Cephalexin 500mg PO BID x 10d (if not anaphylactic), Azithromycin 500mg day 1 then 250mg x 4d, or Clindamycin 300mg PO TID x 10d
Why we treat strep: Primary goal is prevention of rheumatic fever (ARF), not symptom relief. Treatment has up to 9 days from symptom onset to prevent ARF. Antibiotics shorten symptoms by ~1 day and reduce transmission.[10]
When NOT to test: Cough, rhinorrhea, hoarseness, oral ulcers, and conjunctivitis all point toward viral etiology and make strep unlikely. Do not test and do not treat — positive results in this context likely represent carrier state, not true infection.
References
- Galioto NJ. Peritonsillar Abscess. Am Fam Physician. 2017;95(8):501-506. PubMed
- Costantino TG et al. Randomized Trial Comparing Intraoral Ultrasound to Landmark-Based Needle Aspiration in Patients with Suspected Peritonsillar Abscess. Acad Emerg Med. 2012;19(6):626-631. PubMed
- Powell J, Wilson JA. An Evidence-Based Review of Peritonsillar Abscess. Clin Otolaryngol. 2012;37(2):136-145. PubMed
- Chau JK et al. Corticosteroids in Peritonsillar Abscess Treatment: A Blinded Placebo-Controlled Clinical Trial. Laryngoscope. 2014;124(1):97-103. PubMed
- Craig FW, Schunk JE. Retropharyngeal Abscess in Children: Clinical Presentation, Utility of Imaging, and Current Management. Pediatrics. 2003;111(6):1394-1398. PubMed
- Vieira F et al. Deep Neck Infection. Otolaryngol Clin North Am. 2008;41(3):459-483. PubMed
- Bridwell RE et al. Ludwig Angina: An Updated Review and Implications for Emergency Airway Management. Am J Emerg Med. 2021;41:1-5. PubMed
- Baiu I, Melnikow J. Epiglottitis. JAMA. 2019;321(19):1946. PubMed
- Karkos PD et al. Lemierre’s Syndrome: A Systematic Review. Laryngoscope. 2009;119(8):1552-1559. PubMed
- Shulman ST et al. IDSA Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis. Clin Infect Dis. 2012;55(10):e86-102. PubMed
