Last reviewed: March 2026
Contents
MDM Templates
Head Injury — PECARN Low Risk
Child presents after head injury. Using the PECARN pediatric head injury algorithm, patient is negative for all high-risk and intermediate-risk criteria. Well appearing, at neurologic baseline, tolerating oral intake.
If <2 years: No palpable skull fracture, no temporal/parietal/occipital scalp hematoma, no LOC >5 seconds, no severe mechanism of injury, no altered mental status, no abnormal behavior per caregiver.
If ≥2 years: No LOC, no vomiting, no severe mechanism of injury, no severe headache, no signs of basilar skull fracture, no altered mental status.
CT head not recommended per PECARN — risk of clinically important TBI <0.02%. Not consistent with intracranial hemorrhage, skull fracture requiring intervention, or non-accidental trauma based on history and exam.[1]
Plan: Discharge with PCP follow-up in 24-48 hours. Head injury precautions reviewed. Return for vomiting, worsening headache, altered behavior, excessive sleepiness, seizure, or focal neurologic symptoms.
Head Injury — PECARN Intermediate Risk
Child presents after head injury with one or more intermediate-risk PECARN criteria present but no high-risk criteria. GCS 15, at neurologic baseline.
Intermediate risk per PECARN places the child at approximately 1% risk of clinically important TBI. Shared decision making regarding CT versus observation. Factors favoring observation: isolated finding, improving symptoms, experienced clinician comfortable with serial exams, family amenable to close monitoring. Factors favoring CT: multiple intermediate-risk criteria, worsening symptoms, physician or caregiver concern.[1]
Plan: Observation period with serial neurologic exams. If symptoms resolve and child returns to baseline, discharge with head injury precautions and PCP follow-up in 24 hours. If worsening during observation, CT head obtained. Return for same precautions as above.
Blunt Abdominal Trauma
Child presents after blunt abdominal trauma. Hemodynamically stable. Abdominal exam with tenderness but no peritoneal signs, no distention, no seat belt sign.
History and exam lower concern for significant intra-abdominal injury requiring operative intervention. Not consistent with hollow viscus perforation (no peritoneal signs), hemodynamically significant solid organ injury (stable vitals), or free fluid (benign exam). If seat belt sign present, concern for bowel injury is elevated and serial exams warranted even with negative CT.[2]
Plan: Serial abdominal exams. Labs if moderate mechanism. CT abdomen/pelvis with IV contrast if clinical concern warrants imaging. Disposition based on clinical trajectory.
If hemodynamically unstable despite 40 mL/kg crystalloid: Transfuse 10-20 mL/kg pRBCs. Pediatric surgery consulted emergently. Unstable after >40 mL/kg blood products warrants operative intervention.
Non-Accidental Trauma Concern
Child presents with injury pattern inconsistent with stated mechanism. Features raising concern for non-accidental trauma include: injury incompatible with developmental stage, delay in seeking care, inconsistent or changing history between caregivers, injuries in non-mobile infant, bruising in non-cruising child, or patterned injuries.
History and exam raise concern for inflicted injury. Not consistent with accidental mechanism given the clinical findings. Non-accidental trauma must be investigated to prevent further harm to this child and any siblings in the home.[3]
Plan: Full evaluation including skeletal survey, CT head (if <6 months or concern for head injury), LFTs and lipase (occult abdominal injury screening), UA. Social work and child protective services notified. Admit for safety and completion of workup if needed. All findings documented objectively without accusatory language.
Clinical Education
PECARN Decision Rule
The PECARN rule is the most validated clinical decision tool for pediatric head injury. It identifies children at very low risk (<0.02%) of clinically important TBI who do not need CT. Derived from >42,000 children and validated prospectively. Sensitivity approaches 100% for clinically important TBI.[1]
| Criteria | <2 Years | ≥2 Years |
| CT recommended | GCS <15, palpable skull fracture, AMS | GCS <15, signs of basilar skull fracture, AMS |
| Observation vs CT | Non-frontal scalp hematoma, LOC ≥5 sec, severe mechanism, not acting normally | LOC, vomiting, severe mechanism, severe headache |
| CT not recommended | None of the above | None of the above |
Severe mechanism of injury: MVC with ejection, death of another passenger, or rollover. Pedestrian or bicyclist without helmet struck by motorized vehicle. Fall >3 feet (<2 years) or >5 feet (≥2 years). Head struck by high-impact object.
Isolated LOC does not independently predict clinically important TBI. A child with isolated brief LOC and no other risk factors can be safely observed rather than scanned.[1]
Concussion Management
Concussion is a clinical diagnosis. CT is normal in concussion by definition — its role is to exclude intracranial hemorrhage, not to diagnose concussion. Symptoms include headache, dizziness, nausea, confusion, memory difficulty, and emotional lability. Symptoms may be delayed hours after injury.
Acute management: 1-2 days of relative cognitive and physical rest (brain and eye rest — sleep, music, reduced screen time). Complete bed rest beyond 48 hours is counterproductive and delays recovery. Graduated return to activity guided by symptom resolution.[1]
Return to school before return to sport. Cognitive rest is prioritized. No return to contact sport until fully asymptomatic at rest AND during exertion, and cleared by a provider experienced in concussion management. Second impact syndrome (rare but catastrophic) occurs when a second concussion is sustained before full recovery from the first.
Abdominal Trauma Pearls
The seat belt sign (abdominal wall contusion) is a red flag for hollow viscus injury. Small bowel perforation may be present even with a negative CT. Patients with a seat belt sign should be admitted for serial abdominal exams regardless of initial imaging. Also consider Chance fracture (lumbar flexion-distraction injury) in any child with a seat belt sign.[2]
Most pediatric solid organ injuries (liver, spleen, kidney) are managed nonoperatively. Hemodynamic stability determines management, not CT grade. Splenic injuries requiring <40 mL/kg blood in the first 24 hours typically do not need surgery. Liver injuries have a lower threshold (>30 mL/kg) given higher re-bleeding risk.
Isolated microscopic hematuria (<50 RBC/HPF) with suspected renal contusion can be observed without imaging in a stable child. Gross hematuria warrants CT. Kidney injuries are almost always managed conservatively.
Pediatric pelvic fractures rarely cause significant hemorrhage unlike adults. If a child with a pelvic fracture is hypotensive, look for another bleeding source (solid organ injury, intracranial hemorrhage).
C-Spine and SCIWORA
SCIWORA (Spinal Cord Injury Without Radiographic Abnormality) occurs because the pediatric spine has greater ligamentous laxity than the spinal cord can tolerate. A normal radiograph does NOT exclude spinal cord injury in a child. Ask specifically about transient paresthesias at the time of injury — approximately half of patients with delayed-onset SCIWORA have this finding.[2]
Do not force immobilization on a young, alert child with no obvious injuries who is vigorously resisting — forced restraint can cause secondary injuries. Clinical clearance of the c-spine in young children relies on exam (midline tenderness, neurologic deficits, distracting injuries) and mechanism rather than the NEXUS/Canadian C-Spine rules, which are validated for adults.
Non-Accidental Trauma
Bruising in a non-cruising child is abuse until proven otherwise. Infants who cannot pull to stand should not have bruises. The TEN-4 rule identifies high-specificity locations for inflicted bruising: torso, ears, neck in children <4 years, and any bruising in infants <4 months.[3]
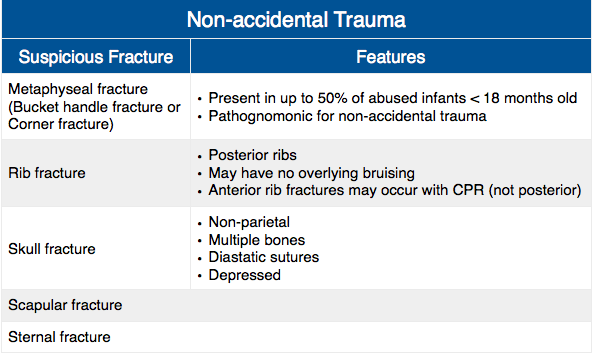
Classic fracture patterns concerning for NAT: metaphyseal corner (“bucket handle”) fractures, posterior rib fractures, multiple fractures in different stages of healing, spiral fractures in non-ambulatory children, and complex skull fractures. Skeletal survey is mandatory in any child <2 years with suspected abuse.
Retinal hemorrhages in an infant with altered mental status are highly specific for abusive head trauma (formerly “shaken baby syndrome”). CT head showing subdural hematomas of different ages further supports the diagnosis. Ophthalmologic exam is part of the standard NAT workup.
Document objectively. Record findings factually (“3 cm circular bruise on left upper arm”) without conclusions about causation. Report concerns to child protective services — this is mandatory, not discretionary. The physician’s role is to identify and report, not to investigate or adjudicate.
Disposition
Admit: Any intracranial hemorrhage on CT. GCS <15 or not at baseline. Significant solid organ injury. Hemodynamic instability. Seat belt sign (for serial exams). Suspected non-accidental trauma (for safety and workup completion). Multisystem trauma.
Discharge: PECARN low-risk head injury. Concussion at baseline with reliable follow-up. Minor abdominal trauma with benign serial exams. Isolated extremity injuries after appropriate imaging. Return for vomiting, worsening headache, altered behavior, abdominal pain, or any new neurologic symptoms.
References
- Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study (PECARN). Lancet. 2009;374(9696):1160-1170. PubMed
- Holmes JF, Lillis K, Monroe D, et al. Identifying children at very low risk of clinically important blunt abdominal injuries. Ann Emerg Med. 2013;62(2):107-116. PubMed
- Christian CW, Committee on Child Abuse and Neglect, AAP. The evaluation of suspected child physical abuse. Pediatrics. 2015;135(5):e1337-e1354. PubMed
