Last reviewed: March 2026
Contents
MDM Templates
Anaphylaxis
Patient presents with acute multisystem allergic reaction involving cutaneous findings and respiratory compromise / cardiovascular instability / gastrointestinal symptoms consistent with anaphylaxis. They deny isolated drug reaction without systemic features. They are being actively resuscitated with airway intact, no uvular or laryngeal edema.
History and exam are consistent with anaphylaxis based on acute onset of multiorgan involvement after allergen exposure. History, exam, and response to treatment lower suspicion for isolated asthma exacerbation, vasovagal syncope, panic attack, systemic mastocytosis, carcinoid, or sepsis.
Plan: Epinephrine 0.3-0.5 mg IM (repeated as needed), methylprednisolone 125 mg IV, diphenhydramine 50 mg IV, famotidine 20 mg IV, IV crystalloid resuscitation, ondansetron 4 mg IV for nausea.
Disposition: Observation minimum 4 hours post last epinephrine dose. If no recurrence of symptoms and tolerating PO, discharge with EpiPen prescription, diphenhydramine 25 mg PO q8h x 3 days, and return precautions for recurrent swelling, dyspnea, or lightheadedness. PCP follow-up within 48 hours. Allergy referral recommended.
Refractory anaphylaxis (no response to 2+ IM doses):
Epinephrine infusion 0.1 mcg/kg/min IV, titrate to effect. Aggressive crystalloid resuscitation. Consider vasopressin if refractory hypotension. Admit to ICU.
Allergic Reaction
Patient presents with acute-onset diffuse urticarial rash. They deny dyspnea, throat tightness, lightheadedness, vomiting, or diarrhea. They are well appearing with no angioedema, no wheezing, and hemodynamically stable.
Presentation is consistent with isolated allergic reaction / urticaria without multisystem involvement. History and exam lower suspicion for anaphylaxis, angioedema requiring airway intervention, vasculitis, drug reaction with systemic features (SJS/TEN), or new-onset systemic mastocytosis.
Plan: Diphenhydramine 25-50 mg PO, prednisone 40-60 mg PO daily x 3 days for significant urticaria.
Disposition: Discharge with return precautions for lip/tongue swelling, difficulty breathing, lightheadedness, or rash progression despite treatment. PCP follow-up within 48 hours.
Clinical Education
Anaphylaxis Diagnostic Criteria
Anaphylaxis is a clinical diagnosis. The 2020 WAO/EAACI updated criteria simplified the definition: anaphylaxis is likely when acute onset (minutes to hours) of illness with involvement of skin/mucosa AND at least one of respiratory compromise, hypotension, or end-organ dysfunction.[1] The prior three-criteria system (NIAID 2006) remains useful as a cognitive framework:
| Criterion | Definition |
| 1 | Skin/mucosal involvement PLUS respiratory OR cardiovascular compromise |
| 2 | Known allergen exposure + 2 or more organ systems involved (skin, respiratory, GI, cardiovascular) |
| 3 | Hypotension alone after known allergen exposure |
Key pearl: Up to 20% of anaphylaxis cases present WITHOUT skin findings. Hypotension or bronchospasm after allergen exposure is anaphylaxis until proven otherwise, even without urticaria.[1]
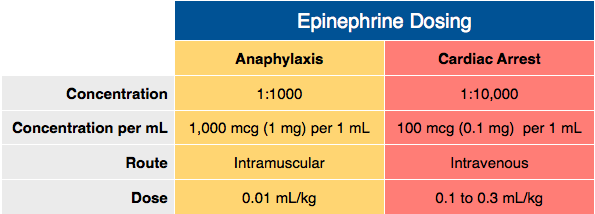
Epinephrine Dosing
IM epinephrine is first-line, always. Give 0.3-0.5 mg of 1:1,000 (1 mg/mL) IM into the anterolateral thigh. Repeat every 5-15 minutes as needed. There is no maximum number of IM doses — if the patient needs it, give it.[2]
IV epinephrine for refractory cases: If 2+ IM doses fail, switch to IV. Start an infusion at 0.1 mcg/kg/min and titrate. Avoid IV push epinephrine in anaphylaxis unless the patient is in arrest — push-dose epi in a patient with a pulse risks dysrhythmia and hypertensive crisis.[2]
Pediatric dosing: 0.01 mg/kg IM (max 0.3 mg in prepubertal children, 0.5 mg in adolescents).
Observation Period & Biphasic Reactions
Biphasic reactions occur in 1-20% of cases (most studies cluster around 5%), typically within 4-8 hours of the initial reaction but occasionally up to 72 hours later.[3] The traditional 4-6 hour observation period after the last epinephrine dose is reasonable for most patients. Longer observation (12-24 hours) is warranted for patients who required multiple epinephrine doses, had refractory hypotension, or have a history of biphasic reactions.
The practical approach: Reassess at 4 hours post last epinephrine. If the patient looks good, is tolerating PO, and has no residual symptoms, the drug is cleared and they can go home. If they’re not back to baseline, extend the observation — the patient is telling you the answer.
Role of Steroids
Steroids do not treat acute anaphylaxis. They have no proven benefit for preventing biphasic reactions, despite decades of routine use. A 2022 Cochrane review found no RCTs supporting glucocorticoids for anaphylaxis prevention or treatment.[4] That said, most emergency physicians still give them because the theoretical benefit is plausible and the harm is minimal for a short course. Just don’t let steroids distract from the only drug that matters: epinephrine.
H1 and H2 blockers (diphenhydramine + famotidine) treat urticaria and may reduce some cutaneous symptoms but do not treat the life-threatening cardiovascular or respiratory components. They are adjuncts, not substitutes for epinephrine.[2]
Contrast Allergy Premedication
For emergent CT with contrast in a patient with reported contrast allergy: Give hydrocortisone 200 mg IV + diphenhydramine 50 mg IV, ideally 1 hour prior but can be given immediately before if the scan is urgent. Modern low-osmolar contrast has a much lower reaction rate (~0.2-0.7%) than older ionic contrast.[5]
Important nuance: “Iodine allergy” is a misnomer — the reaction is to the contrast molecule, not iodine itself. Shellfish allergy does not increase contrast reaction risk. The strongest risk factor for a contrast reaction is a prior contrast reaction.[5]
References
- Cardona V et al. World Allergy Organization Anaphylaxis Guidance 2020. World Allergy Organ J. 2020;13(10):100472. PubMed
- Shaker MS et al. Anaphylaxis — A 2020 Practice Parameter Update, Systematic Review, and GRADE Analysis. J Allergy Clin Immunol. 2020;145(4):1082-1123. PubMed
- Lee S et al. Biphasic Anaphylaxis: Review of Incidence, Clinical Predictors, and Observation Recommendations. Immunol Allergy Clin North Am. 2015;35(2):313-326. PubMed
- Liyanage CK et al. Glucocorticoids for the Treatment of Anaphylaxis. Cochrane Database Syst Rev. 2022;(3):CD007596. PubMed
- ACR Committee on Drugs and Contrast Media. ACR Manual on Contrast Media. 2024. ACR
