Last reviewed: March 2026Contents
MDM Templates
Acute Otitis Media (AOM)
Exam and history most consistent with AOM.
I do not see evidence at this time for mastoiditis, malignant otitis externa, herpes, retained foreign body.
Rx: Wait-and-see antibiotic prescription Amoxicillin 45mg/kg BID x 7 days
Disposition: Discharge. If symptoms worsen or persist for 48-72 hours then patient to fill the prescription. Cautious return precautions discussed with full understanding.
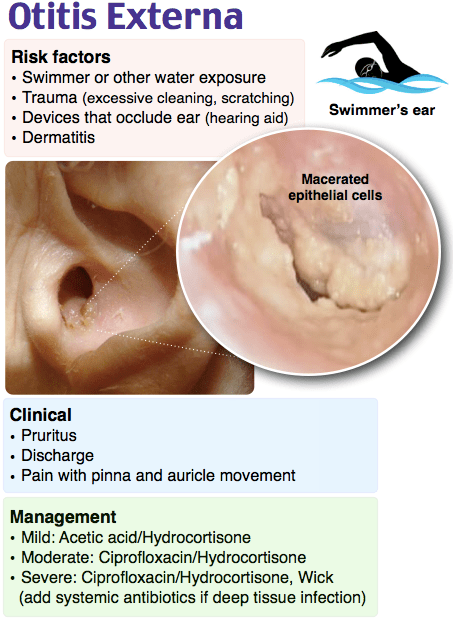
Otitis Externa
Exam and history are most consistent with Otitis Externa.
No diabetes, immunosuppression.
Low suspicion for mastoiditis, malignant otitis externa, AOM, herpes.
Rx: CiproDex 4 drops instilled into the affected ear twice daily for seven days.
Disposition: Discharge home. Return precautions discussed. Advise follow up with primary care provider within 24-48 hours.
Mastoiditis
Patient presenting with fever, otalgia, pain, and erythema posterior to the ear.
Presentation most consistent with Mastoiditis.
Interventions:
- IV antibiotics (see below*)
- IVF resuscitation
- ENT consultation
Disposition: Admit for continued antibiotics and monitoring for complications such as meningitis, brain abscess, sinus thrombosis, nerve palsy.
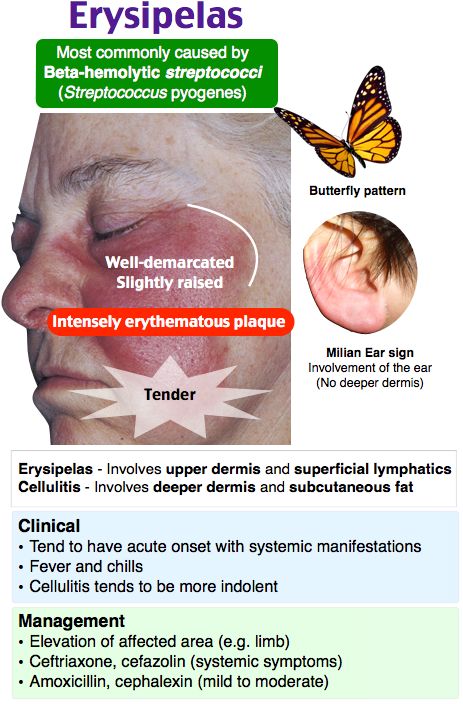
Perichondritis
Exam and history are most consistent with auricular perichondritis.
No diabetes, immunosuppression.
Low suspicion for erysipelas, abscess, mastoiditis, malignant otitis externa, AOM, herpes.
Rx: Ciprofloxacin 500mg PO BID x 7-10 days and removal of offending agent (piercing).
Disposition: Discharge with close follow up for recheck to ensure no perichondrial abscess development.
Clinical Education
AOM Pearls
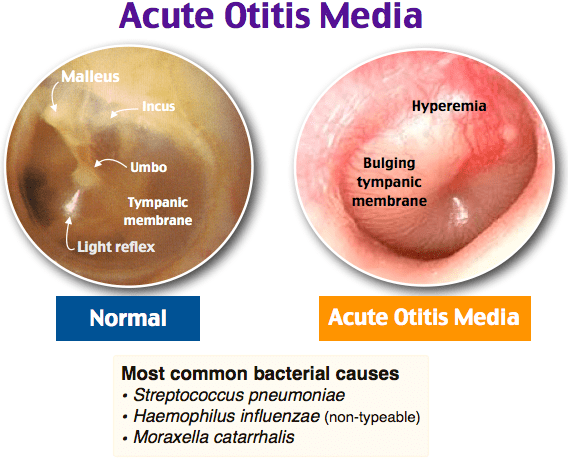
Watch-and-wait vs immediate antibiotics: AAP guidelines support observation with a safety-net prescription for children ≥6 months with unilateral, non-severe AOM. Immediate antibiotics for: age <6 months, bilateral AOM in children <2 years, severe symptoms (moderate-severe otalgia, fever ≥39°C), otorrhea, or immunocompromised.[1]
Antibiotic selection:
- 1st line: Amoxicillin 45mg/kg BID x 7-10 days (adults: 500mg TID)
- 2nd line (treatment failure or recent abx): Amoxicillin-clavulanate 90mg/kg/day (high-dose) or Cefdinir 7mg/kg PO BID x 10 days
- 3rd line: Clindamycin
- IM option: Ceftriaxone 50mg/kg IM x1 if unable to tolerate PO — can discharge with oral abx to attempt or PCP follow up within 24 hours
TM rupture with AOM: Can still treat with oral amoxicillin. Some add topical Cortisporin (neomycin/polymyxin/hydrocortisone) Suspension (NOT Solution — solution is ototoxic through a perforation).[2]
Complications to watch for: Lateral sinus thrombosis (AOM refractory to treatment + 6th nerve palsy), mastoiditis (post-auricular erythema/swelling), intracranial abscess. These are reasons for CT temporal bone and ENT consultation.
Otitis Externa Pearls
Treatment ladder:
| Severity | Treatment |
| Super mild | 2% acetic acid solution + hydrocortisone drops |
| Mild-moderate | Cortisporin (neomycin/polymyxin/hydrocortisone) solution 4 drops QID x 7 days. Use Suspension if TM perforation. |
| Moderate-severe | CiproDex 4 drops BID x 7 days OR Ciprofloxacin otic + hydrocortisone drops. Add ear wick if canal too edematous for drops to penetrate. |
Ear wick: Insert when the canal is too swollen for drops to penetrate. The wick expands with the drops and keeps medication in contact with the canal wall. Remove or replace at 48-72 hour follow-up.[3]
Keep it dry: Advise no swimming, avoid water in the ear during bathing (cotton ball with petroleum jelly). Water exposure is the #1 modifiable risk factor for recurrence.
Malignant (Necrotizing) Otitis Externa
Who gets it: Elderly diabetics and immunocompromised patients. Pseudomonas aeruginosa almost always the causative organism.[4]
Why it’s dangerous: Infection invades from the ear canal into the temporal bone → skull base osteomyelitis. Can spread to cause cranial nerve palsies (facial nerve VII most common, then IX, X, XI, XII), sigmoid sinus thrombosis, meningitis, and brain abscess. Mortality 10-20% even with treatment.[4]
Red flags: Otalgia out of proportion to exam, granulation tissue at the bony-cartilaginous junction of the ear canal floor, cranial nerve deficits, failure to improve with standard OE treatment in a diabetic/immunocompromised patient.
Workup: CT temporal bone (look for bony erosion), ESR/CRP (elevated, useful for monitoring treatment response). MRI for intracranial extension if concern for CN involvement.
Treatment: Ciprofloxacin 400mg IV BID (or 750mg PO BID if mild and reliable follow-up) for 6-8 weeks. ENT consult for debridement. Always admit if IV antibiotics needed.[4]
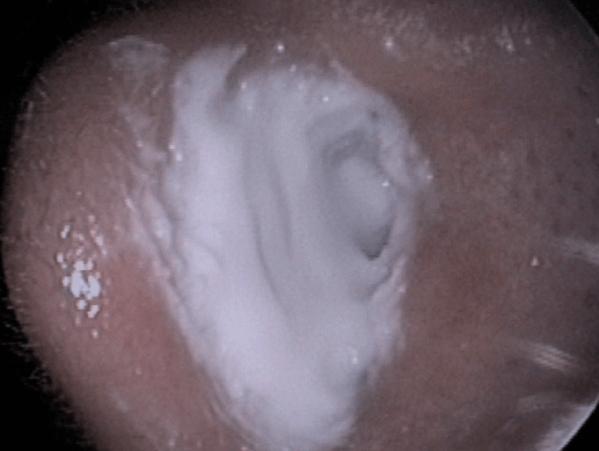
Otomycosis
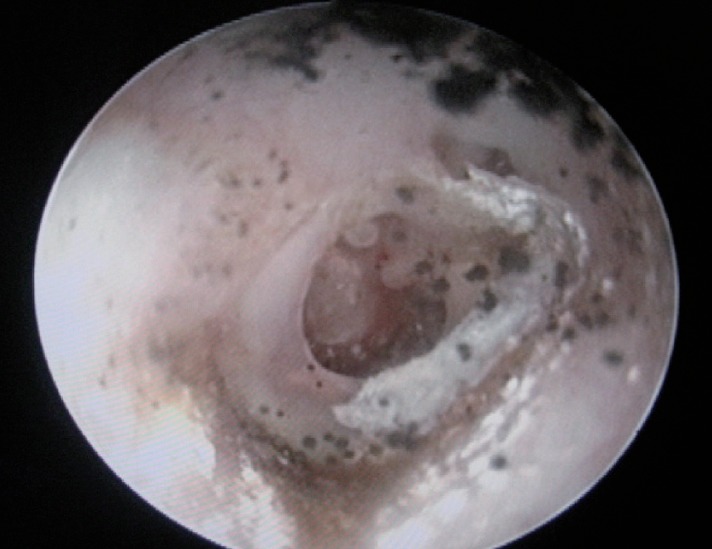
What it looks like: Fluffy white/black fungal debris in the ear canal, often with wet newspaper or blotting paper appearance. Usually Aspergillus or Candida. Suspect when OE fails standard antibacterial drops or after prolonged antibiotic drop use.[5]
Treatment options:
- Approach 1: 1% clotrimazole solution 4 drops QID x 7 days
- Approach 2: 1% clotrimazole solution on cotton-tipped applicators applied to ears BID
- Approach 3: 1% clotrimazole cream x1 filling the external auditory meatus after cleaning in the ED
TM perforation: Clotrimazole is safe with perforated TMs. Some sources suggest aqueous miconazole 0.5% as an alternative with perforation.[5]
Mastoiditis Pearls
Presentation: Post-auricular erythema, swelling, and tenderness with protrusion of the auricle anteriorly and inferiorly. Usually follows or accompanies AOM. Children most commonly affected.[6]
Imaging: CT temporal bone with IV contrast — look for coalescent mastoiditis (destruction of bony septae), subperiosteal abscess, or intracranial extension.
See: Radiopaedia — Acute Mastoiditis CT examples
Antibiotics:
- Standard: Clindamycin 600mg IV q8h (covers most AOM pathogens including MRSA)
- MRSA risk or severe: Ceftriaxone 1g IV (50mg/kg peds) + Vancomycin 15-20mg/kg IV
Complications: Subperiosteal abscess (most common surgical complication), Bezold abscess (tracking along SCM into the neck), sigmoid sinus thrombosis, epidural/brain abscess, meningitis, facial nerve palsy.[6]
Disposition: Always admit. ENT consult — may need myringotomy with tube placement or mastoidectomy if abscess or failure to improve on IV antibiotics.
Perichondritis Pearls
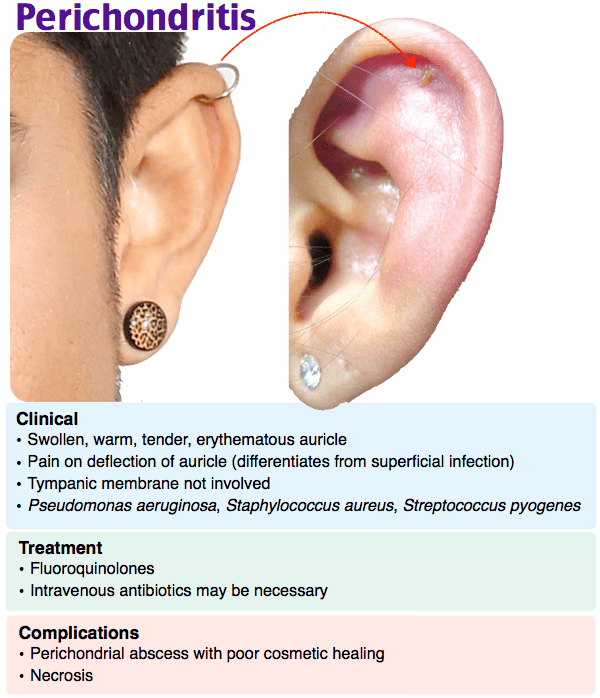
Etiology: Most commonly from ear piercings (especially high cartilage piercings), trauma, or extension from OE. Pseudomonas is the most common pathogen — standard cephalosporins won’t cover it.[7]
Key exam finding: Erythema and swelling of the auricle that spares the lobule (the lobule has no cartilage). If the lobule is involved, think cellulitis/erysipelas instead.
Treatment: Fluoroquinolone required for Pseudomonas coverage — Ciprofloxacin 500mg PO BID x 7-10 days. Remove any foreign body (piercing). If fluctuant, I&D of perichondrial abscess with bolster dressing to prevent reaccumulation.
Why it matters: Untreated perichondritis → cartilage necrosis → permanent “cauliflower ear” deformity. Despite treatment, auricle necrosis and permanent cartilage damage can still occur, so close follow-up is important.[7]
Tympanic Membrane Perforation
Causes: Trauma (Q-tip, blast injury, slap), AOM with rupture, barotrauma (diving, flying).
Management: Most traumatic perforations heal spontaneously within 2-3 months. Keep ear dry. No ototoxic drops (aminoglycosides) through a perforation — use fluoroquinolone otic drops (ofloxacin, ciprofloxacin) if treatment needed.[8]
ENT referral indications: Perforation >50% of TM, associated ossicular disruption (significant conductive hearing loss), no healing by 3 months, perforation involving the TM margin.
Drop safety with perforations:
| Safe through perforation | Ototoxic — avoid with perforation |
| Ofloxacin otic, Ciprofloxacin otic, Cortisporin Suspension | Cortisporin Solution, Gentamicin otic, Neomycin-containing solutions |
Ear Foreign Body
Approach: Visualize with otoscope first. Irrigation is first-line for most non-organic FBs — do NOT irrigate if organic material (beans, seeds — they swell), button battery, or known TM perforation.[9]
Button battery: True emergency — can cause liquefactive necrosis of the ear canal within hours. Remove immediately. ENT if not easily retrievable.
Live insect: Kill it first with mineral oil, 2% lidocaine, or microscope immersion oil instilled into the canal. Then remove with irrigation or alligator forceps. A live insect is extremely distressing to the patient and attempts at blind removal can push it further in.[9]
When to stop and call ENT: Failed 2-3 attempts, uncooperative child, FB medial to the isthmus (high risk of canal/TM injury), button battery you can’t easily grab, or any concern for TM injury during removal.
References
- Lieberthal AS et al. The Diagnosis and Management of Acute Otitis Media. Pediatrics. 2013;131(3):e964-e999. PubMed
- Rosenfeld RM et al. Clinical Practice Guideline: Acute Otitis Externa. Otolaryngol Head Neck Surg. 2014;150(1 Suppl):S1-S24. PubMed
- Kaushik V et al. Interventions for Acute Otitis Externa. Cochrane Database Syst Rev. 2010;(1):CD004740. PubMed
- Carfrae MJ, Kesser BW. Malignant Otitis Externa. Otolaryngol Clin North Am. 2008;41(3):537-549. PubMed
- Anwar K, Gohar MS. Otomycosis; Clinical Features, Predisposing Factors and Treatment Implications. Pak J Med Sci. 2014;30(3):564-567. PubMed
- Loh R et al. Mastoiditis — A Review of a Common Condition with an Uncommon Complication. J Pediatr. 2018;198:263-267. PubMed
- Davidi E et al. Perichondritis of the Ear — Analysis of 10 Cases. Isr Med Assoc J. 2011;13(1):21-24. PubMed
- Lou ZC et al. Traumatic Tympanic Membrane Perforations: A Study of Etiology and Factors Affecting Outcome. Am J Otolaryngol. 2012;33(5):549-555. PubMed
- Heim SW, Maughan KL. Foreign Bodies in the Ear, Nose, and Throat. Am Fam Physician. 2007;76(8):1185-1189. PubMed
