Last reviewed: March 2026Contents
MDM Templates
Bell’s Palsy — Within 72 Hours
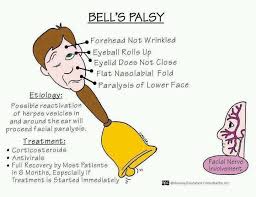
Patient presents with acute onset unilateral facial weakness involving the forehead, eye, and mouth — consistent with a peripheral (lower motor neuron) pattern.
Symptom onset was within the last *** hours/days.
They deny vesicular rash on the ear or palate, hearing changes, limb weakness, diplopia, dysphagia, and dysarthria.
No recent tick exposure or erythema migrans.
No history of immunosuppression.
Exam demonstrates
*** (describe: Incomplete eye closure, flattened nasolabial fold, inability to raise eyebrow).
Importantly, the forehead is involved — this is NOT a forehead-sparing pattern.
No vesicles on the ear, external auditory canal, or palate. Otoscopic exam is normal. Remainder of cranial nerve exam is intact. No limb weakness, ataxia, or other focal neurologic deficits.
History and exam lower suspicion for stroke (no forehead sparing, no other focal deficits), Ramsay Hunt syndrome (no vesicular rash or otalgia), Lyme disease (no tick exposure, no rash, low-endemic area), parotid or skull base mass (acute onset), and other central or infectious etiologies. Clinical presentation is most consistent with Bell’s palsy (idiopathic peripheral facial nerve palsy).
Plan:
– Prednisone 60 mg daily for 7 days, started today (within 72-hour window).[1]
– Eye protection with artificial tears every 1-2 hours while awake and lubricating ophthalmic ointment at bedtime. Patient instructed to tape eye shut at night if unable to fully close.
Disposition: Discharge with PCP follow-up within 1 week. Return precautions for worsening weakness, new limb weakness or numbness, vesicular rash on the ear, difficulty swallowing, vision changes, or no improvement after 3 weeks. If incomplete recovery at 3 months, may need referral to ophthalmology and/or facial nerve specialist.
If severe (House-Brackmann V-VI — near-total or total paralysis): Given severity of paralysis, adding valacyclovir 1000 mg TID for 7 days in combination with prednisone. Evidence for antivirals is limited, but potential benefit is highest in severe cases.[2]
Bell’s Palsy — Late Presentation
Patient presents with unilateral facial weakness with onset *** days ago, now beyond the 72-hour treatment window.
Pattern is peripheral (forehead involved).
They deny vesicular rash, otalgia, tick exposure, limb weakness, and other neurologic symptoms.
Exam demonstrates
*** (describe: Incomplete eye closure, flattened nasolabial fold, inability to raise eyebrow).
Importantly, the forehead is involved — this is NOT a forehead-sparing pattern.
No vesicles on the ear, external auditory canal, or palate. Otoscopic exam is normal. Remainder of cranial nerve exam is intact. No limb weakness, ataxia, or other focal neurologic deficits.
History and exam lower suspicion for stroke, Ramsay Hunt syndrome, Lyme disease, and mass lesion. Presentation is consistent with Bell’s palsy. Given that onset was more than 72 hours ago, the benefit of corticosteroids is uncertain — strong evidence for steroids exists only when initiated within 72 hours.[1]
Plan: Eye protection with artificial tears every 1-2 hours while awake and lubricating ointment at bedtime. *** (consider steroids on case-by-case basis if still within 7 days of onset, discuss with patient).
Disposition: Discharge with PCP follow-up within 1 week. Same return precautions as above. If no improvement by 3 weeks or worsening after initial improvement, recommend urgent neurology referral to evaluate for alternative diagnoses.
Ramsay Hunt Syndrome
Patient presents with acute unilateral facial weakness with associated otalgia and vesicular eruption on the *** (ear/external auditory canal/palate/tongue). This triad is consistent with Ramsay Hunt syndrome (herpes zoster oticus) — VZV reactivation in the geniculate ganglion.[3]
Exam demonstrates peripheral facial palsy (House-Brackmann grade ***) with vesicles visible on ***.
*** (hearing changes, vestibular symptoms if present).
No other cranial nerve deficits.
No limb weakness or ataxia.
History and exam lower suspicion for stroke, otitis media/externa with complications, parotid pathology, and Lyme disease.
Plan: Prednisone 60 mg daily for 7 days AND valacyclovir 1000 mg TID for 7 days — antivirals are standard of care in Ramsay Hunt (unlike typical Bell’s palsy).[3] Eye protection as above. Pain management with ***.
Disposition: Discharge with PCP follow-up within 1 week. Patient counseled that Ramsay Hunt has a worse prognosis than typical Bell’s palsy — complete recovery occurs in approximately 50-70% of cases. ENT or neurology referral if hearing loss or vestibular symptoms are present. Return precautions for worsening pain, new hearing loss, vertigo, difficulty swallowing, or signs of secondary infection.
Clinical Education
Central vs Peripheral Facial Palsy
This is the single most important distinction in the ED evaluation of facial weakness. Getting it wrong means missing a stroke.
| Feature | Peripheral (LMN) — Bell’s Palsy | Central (UMN) — Stroke |
| Forehead | Involved — cannot raise eyebrow, wrinkle forehead | SPARED — can raise eyebrow and wrinkle forehead |
| Eye closure | Weak or absent — Bell’s phenomenon (eye rolls up on attempted closure) | Usually preserved |
| Distribution | Entire ipsilateral face (upper + lower) | Contralateral lower face only |
| Other neuro deficits | None (isolated CN VII) | Often present — arm/leg weakness, speech, ataxia |
| Next step | Clinical diagnosis, treat as Bell’s palsy | Stroke workup — CT/CTA, consider tPA, neurology |
Why is the forehead spared in central lesions? The forehead portion of the facial motor nucleus receives bilateral cortical input (from both hemispheres). A unilateral cortical or corticobulbar lesion knocks out only one side of input — the contralateral hemisphere still innervates the forehead. The lower face receives only contralateral input, so it’s affected.[4]
Caveat: A small pontine stroke can cause a peripheral-pattern facial palsy (lesion at the facial nucleus or fascicle). If the patient has ANY other brainstem signs — diplopia, vertigo, ataxia, dysarthria, Horner’s, contralateral weakness — get imaging regardless of forehead involvement.
Radiopaedia: Facial Nerve Anatomy
Dangerous Mimics
Bell’s palsy is a diagnosis of exclusion. Before labeling a patient with Bell’s palsy, actively rule out these mimics — several are time-sensitive emergencies.
| Mimic | Key distinguishing features | Action |
| Stroke | Forehead SPARED (central pattern). Other focal deficits: arm/leg weakness, dysarthria, ataxia, visual field cut. Pontine strokes can mimic peripheral pattern but will have other brainstem signs. | CT/CTA stat. Neurology consult. Consider tPA if within window. |
| Ramsay Hunt syndrome | Vesicles on ear, EAC, or palate. Severe otalgia. May have hearing loss or vertigo (CN VIII involvement). Vesicles may appear AFTER facial palsy onset — re-examine the ear closely.[3] | Steroids + antivirals. ENT if hearing loss. |
| Lyme disease | Endemic area. Tick exposure. Erythema migrans (may have resolved). Bilateral facial palsy is highly suggestive. May have arthritis, AV block, meningismus.[5] | Lyme serology. Doxycycline. Avoid steroids if Lyme suspected. |
| Otitis media / mastoiditis | Ear pain, otorrhea, fever, abnormal TM. Facial palsy from middle ear infection spreading to facial nerve canal. Mastoid tenderness. | CT temporal bone. ENT consult. IV antibiotics. |
| Malignant otitis externa | Diabetic or immunocompromised patient. Severe ear pain out of proportion. Granulation tissue in EAC. Facial palsy is a late and ominous sign. | CT temporal bone. ENT consult. IV anti-pseudomonal antibiotics. |
| Parotid tumor | Gradual onset (weeks to months). Palpable parotid mass. May affect individual branches rather than entire nerve. | CT or MRI with contrast. ENT/surgery referral. |
| Guillain-Barré syndrome | Bilateral facial weakness (facial diplegia variant). Ascending weakness, areflexia, paresthesias. Recent viral illness. May present with facial palsy before limb involvement.[6] | LP, nerve conduction studies. Neurology consult. Admit — risk of respiratory failure. |
| Sarcoidosis (Heerfordt) | Bilateral facial palsy, parotid swelling, uveitis, fever. Often young African American patients. May be the presenting feature of systemic sarcoid. | CXR (bilateral hilar LAD), ACE level, ophthalmology. |
| Temporal bone fracture | History of trauma. Hemotympanum, Battle sign, CSF otorrhea. Facial palsy may be immediate (nerve transection) or delayed (edema). | CT temporal bone. ENT and neurosurgery consult. |
Red flags that should stop you from diagnosing Bell’s palsy: forehead sparing, bilateral facial weakness, gradual onset (weeks), recurrent episodes, other cranial nerve deficits, limb weakness or sensory changes, vesicular rash, palpable mass, recent trauma, and immunosuppression.
Radiopaedia: Bell’s Palsy | Radiopaedia: Ramsay Hunt Syndrome
House-Brackmann Grading
The House-Brackmann scale standardizes facial nerve function and guides treatment intensity. Grade at the initial ED visit — it predicts prognosis and determines whether to add antivirals.[7]
| Grade | Description | Function |
| I | Normal | Normal symmetric function |
| II | Mild dysfunction | Slight weakness on close inspection. Complete eye closure with minimal effort. |
| III | Moderate dysfunction | Obvious but not disfiguring asymmetry. Complete eye closure with effort. Slight mouth movement with maximal effort. |
| IV | Moderately severe | Obvious weakness and/or disfiguring asymmetry. Incomplete eye closure. Asymmetric mouth with maximal effort. |
| V | Severe dysfunction | Barely perceptible motion. Incomplete eye closure. Slight movement of mouth corner. |
| VI | Total paralysis | No movement at all. |
Treatment implications: Grade II-IV — steroids alone. Grade V-VI — consider adding valacyclovir to steroids given worse prognosis and theoretical benefit in severe cases.[2] Grade IV-VI patients need aggressive eye protection and closer follow-up due to incomplete eye closure.
Treatment: Steroids & Antivirals
Steroids work. Antivirals (for typical Bell’s palsy) probably don’t — at least not alone.
Corticosteroids are the cornerstone of treatment. The landmark Sullivan et al. (2007) NEJM trial showed that prednisolone within 72 hours significantly improved complete recovery (83% vs 64%, NNT ~6).[1] Standard dosing is prednisone 60-80 mg daily for 7 days (some protocols taper over days 8-10, but evidence for taper vs abrupt stop is equivalent). Must be started within 72 hours of symptom onset — there is no evidence of benefit beyond this window.
Antivirals alone have no proven benefit for Bell’s palsy. The same Sullivan trial showed acyclovir alone did not improve outcomes. A 2019 Cochrane review confirmed no benefit of antivirals as monotherapy.[8]
Combined steroids + antivirals: The AAN 2012 guideline rates this as “possibly effective” — the evidence is conflicting, and the added benefit over steroids alone is small at best.[2] Most current EM practice reserves combined therapy for severe cases (House-Brackmann V-VI), where the worse prognosis may justify the marginal potential benefit. If prescribed, use valacyclovir 1000 mg TID for 7 days (better bioavailability than acyclovir).
| Severity | Treatment (within 72h) |
| Mild-moderate (HB II-IV) | Prednisone 60 mg daily × 7 days + eye protection |
| Severe (HB V-VI) | Prednisone 60 mg daily × 7 days + valacyclovir 1000 mg TID × 7 days + eye protection |
| Late presentation (>72h) | Eye protection. Steroids may be considered case-by-case if still within ~7 days, but no strong evidence. |
| Ramsay Hunt | Prednisone 60 mg daily × 7 days + valacyclovir 1000 mg TID × 7 days (antivirals are standard here) |
Ramsay Hunt Syndrome Pearls
Ramsay Hunt is VZV reactivation in the geniculate ganglion — the classic triad is ipsilateral facial palsy + vesicular eruption on the ear/palate + otalgia. However, the full triad is present in only about 50% of cases at initial presentation.[3]
Vesicles may lag behind the facial palsy by days. If a patient has unexplained severe otalgia with facial palsy and no vesicles yet, consider Ramsay Hunt and examine the ear carefully on follow-up. Some cases present as “zoster sine herpete” — VZV reactivation without ever developing visible vesicles, diagnosed by PCR.
Worse prognosis than Bell’s palsy: Complete recovery occurs in only 50-70% of Ramsay Hunt patients (vs ~85% for Bell’s). CN VIII involvement is common, causing sensorineural hearing loss and/or vestibular dysfunction. Other cranial nerves (V, IX, X) can also be affected in severe cases.[3]
Treatment: Steroids + antivirals are both standard for Ramsay Hunt (unlike Bell’s, where antivirals are debatable). Valacyclovir 1000 mg TID × 7 days plus prednisone 60 mg daily × 7 days. Earlier treatment correlates with better outcomes.
Lyme Facial Palsy
In Lyme-endemic areas, Lyme disease should be on the differential for every peripheral facial palsy. Facial palsy is the most common cranial neuropathy of Lyme disease and can be the presenting feature — occurring in early disseminated disease (weeks to months after tick bite).[5]
Bilateral facial palsy is highly suspicious for Lyme. While most Lyme facial palsy is unilateral, Lyme is the leading cause of bilateral facial nerve palsy in endemic areas. The bilateral palsy may be simultaneous or sequential (days apart). Other causes of bilateral facial palsy to consider: GBS, sarcoidosis, and HIV.
Do NOT give steroids if Lyme is suspected. Corticosteroids may impair the immune response needed to clear the Borrelia spirochete. If you suspect Lyme, send serology (ELISA followed by Western blot if positive) and treat with doxycycline 100 mg BID for 21-28 days. If there is diagnostic uncertainty in an endemic area, it is reasonable to start doxycycline and defer steroids until Lyme is ruled out.[5]
Lyme clues: Known tick exposure, erythema migrans rash (may have already resolved), endemic area (Northeast US, upper Midwest, Pacific Northwest), summer/fall season, associated arthritis, AV block, or meningitis symptoms.
Eye Protection
Corneal exposure keratitis is the most common complication of Bell’s palsy and the one thing the ED can directly prevent. The inability to fully close the eye exposes the cornea to drying, ulceration, and potential permanent vision loss.[4]
| Intervention | Details |
| Artificial tears | Every 1-2 hours while awake. Preservative-free preferred if using >4x/day. |
| Lubricating ointment | Apply to affected eye at bedtime (e.g., Lacri-Lube). Ointment blurs vision, so reserved for nighttime. |
| Taping | Tape eye shut at night if incomplete closure (HB IV+). Use paper tape horizontally across the closed lid. |
| Moisture chamber | Wraparound glasses or a clear plastic shield over the eye. Particularly useful in dry or windy environments. |
Perform a slit lamp exam if the patient reports eye pain, redness, tearing, or foreign body sensation — corneal abrasion or early keratitis may already be present. Fluorescein staining will reveal epithelial defects. If keratitis is found, add erythromycin ophthalmic ointment and arrange urgent ophthalmology follow-up.
References
- Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N Engl J Med. 2007;357(16):1598-1607. PubMed
- Gronseth GS, Paduga R; AAN. Evidence-based guideline update: steroids and antivirals for Bell palsy. Neurology. 2012;79(22):2209-2213. PubMed
- Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71(2):149-154. PubMed
- Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell’s palsy. Otolaryngol Head Neck Surg. 2013;149(3 Suppl):S1-S27. PubMed
- Halperin JJ, Shapiro ED, Logigian E, et al. Practice parameter: treatment of nervous system Lyme disease. Neurology. 2007;69(1):91-102. PubMed
- Leonhard SE, Mandarakas MR, Gondim FAA, et al. Diagnosis and management of Guillain-Barré syndrome in ten steps. Nat Rev Neurol. 2019;15(11):671-683. PubMed
- House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2):146-147. PubMed
- Gagyor I, Madhok VB, Daly F, et al. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2019;9(9):CD001869. PubMed
