Last reviewed: March 2026
Contents
MDM Templates
Shoulder Dislocation
Patient presents with shoulder pain and inability to move the affected extremity after injury. Exam demonstrates squared-off glenohumeral joint with arm held in slight abduction and external rotation. Sensation intact over deltoid. Neurovascular exam distally intact.
Imaging confirms glenohumeral dislocation without associated fracture. Dislocation successfully reduced at bedside. Post-reduction imaging confirms anatomic reduction. Neurovascular status intact before and after reduction.
Plan: Sling immobilization. Analgesics.
Disposition: Discharge with return precautions and orthopedic follow-up within 1 week for further evaluation and rehab planning.
Clavicle Fracture
Patient presents with clavicle pain after injury. Imaging confirms clavicle fracture. They do not currently demonstrate complications such as compartment syndrome, neurovascular injury, or pneumothorax. The fracture has been satisfactorily immobilized.
History, exam, and imaging not concerning for open fracture, neurovascular compromise, skin tenting, or significant displacement threatening overlying skin.
Plan: Sling immobilization. Analgesics. Gentle ROM exercises at 2–4 weeks, strengthening at 6–10 weeks.
Disposition: Discharge with return precautions and orthopedic follow-up within 1 week.
If medial third fracture with posterior displacement:
Orthopedics consulted emergently with thoracic surgery on standby given risk of great vessel and airway compromise. No current signs of airway or vascular compromise.
Proximal Humerus Fracture
Patient presents with shoulder pain and inability to move the affected extremity after injury. Imaging demonstrates proximal humerus fracture. They do not currently demonstrate complications such as compartment syndrome, neurovascular injury, or skin tenting. Sensation over deltoid is intact.
Plan: Sling and swathe immobilization. Analgesics.
Disposition: Discharge with return precautions and orthopedic follow-up within 1 week.
If multi-part fracture, significant displacement, or fracture-dislocation:
Orthopedics consulted regarding fracture pattern, need for operative fixation, and disposition.
AC Separation
Patient presents with pain over the AC joint after direct blow or fall onto the shoulder. Exam demonstrates point tenderness over the AC joint with deformity. Neurovascular exam distally intact.
Imaging demonstrates AC separation. History, exam, and workup not consistent with clavicle fracture, glenohumeral dislocation, or neurovascular injury.
Plan: Sling for comfort. Analgesics.
Disposition: Discharge with return precautions and orthopedic follow-up within 1–2 weeks.
Rotator Cuff Injury
Patient presents with shoulder pain and difficulty with overhead movement. Exam consistent with rotator cuff pathology — positive impingement signs, weakness with resisted abduction or external rotation. Neurovascular exam intact. No bony tenderness.
History and exam lower suspicion for fracture, dislocation, and neurovascular injury. Presentation consistent with rotator cuff injury — acute versus chronic degeneration to be determined by outpatient imaging.
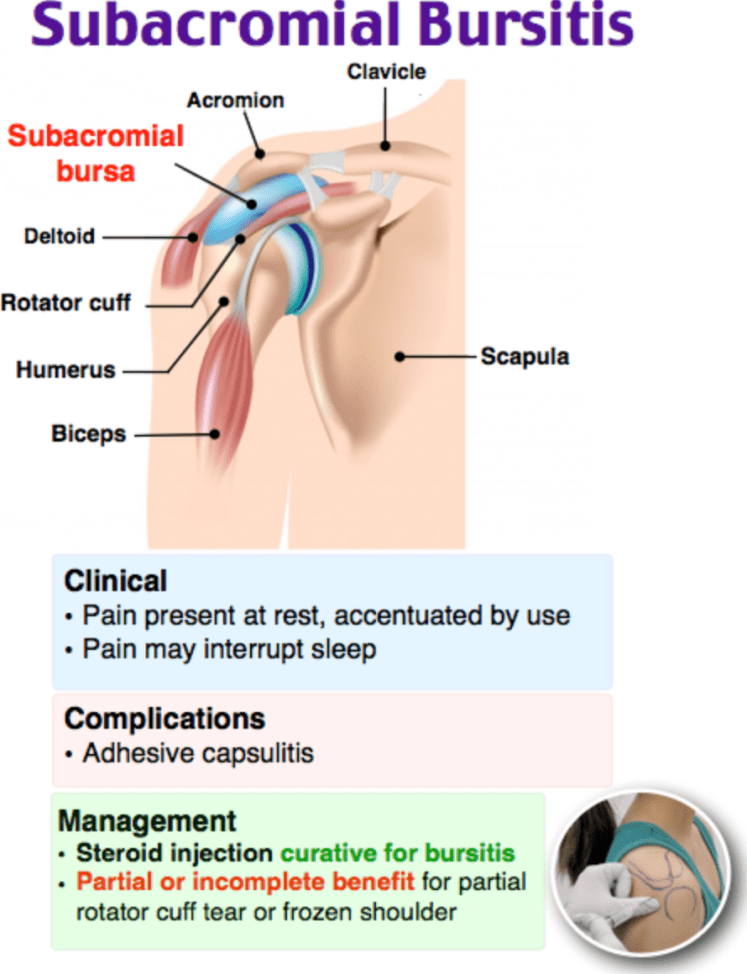
Plan: Sling for comfort. Analgesics. Subacromial injection performed for pain relief.
Disposition: Discharge with return precautions. Follow up with PCP or orthopedics within 1–2 weeks for MRI and further management.
Procedure Notes
Shoulder Reduction
Location: *** shoulder
Time Out: Correct patient, correct procedure confirmed
Consent: Verbal consent obtained
Anesthesia: Procedural sedation with *** / Intra-articular lidocaine 20 mL of 1% injected 2 cm inferior and lateral to the acromion
Position: Supine
Method: *** technique. Gentle traction-countertraction / external rotation / Cunningham / scapular manipulation performed
Post-procedure: Joint appears clinically reduced. Post-reduction X-ray confirms anatomic reduction. Neurovascular status intact before and after reduction
Immobilization: Sling applied
Complications: None. Patient tolerated procedure well.
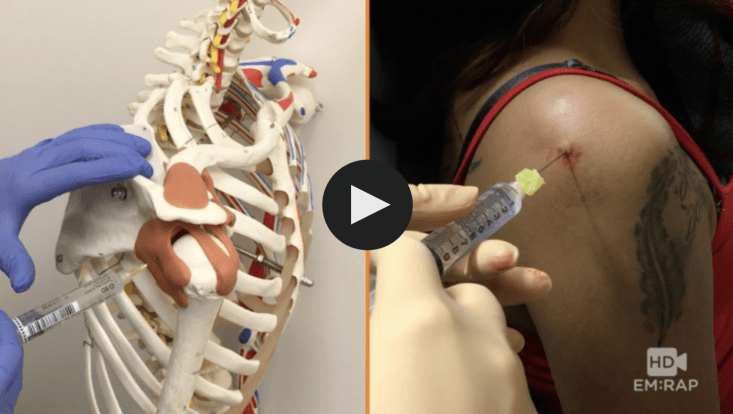
Subacromial Injection
Location: *** shoulder, posterior subacromial approach
Time Out: Correct patient, correct procedure confirmed
Anesthesia: Ethyl chloride spray to skin
Approach: Needle inserted 2 cm inferior and medial to posterolateral corner of acromion, directed toward opposite nipple. Entered subacromial space without resistance
Injection: 3 mL of 1% lidocaine mixed with 40 mg triamcinolone
Complications: None. Patient tolerated procedure well. Significant pain relief noted.
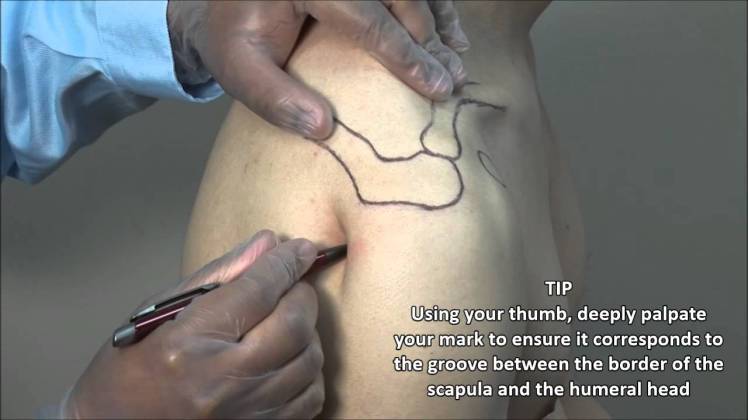
Posterior subacromial injection approach
Injection landmarks
Clinical Education
Shoulder Dislocation Pearls
Check axillary nerve function before and after reduction. Test sensation over the lateral deltoid (regimental badge area). Axillary nerve injury occurs in ~5% of anterior dislocations, more commonly in older patients. Document it pre-reduction so post-reduction deficits aren’t attributed to your reduction.[1]
Intra-articular lidocaine is an underused alternative to procedural sedation. Inject 20 mL of 1% lidocaine into the glenohumeral joint (2 cm inferior and lateral to the acromion, directed posteriorly). Wait 15 minutes, then reduce. Success rates are comparable to sedation for first-time dislocations, and it avoids the recovery time and resource requirements of sedation.[2]
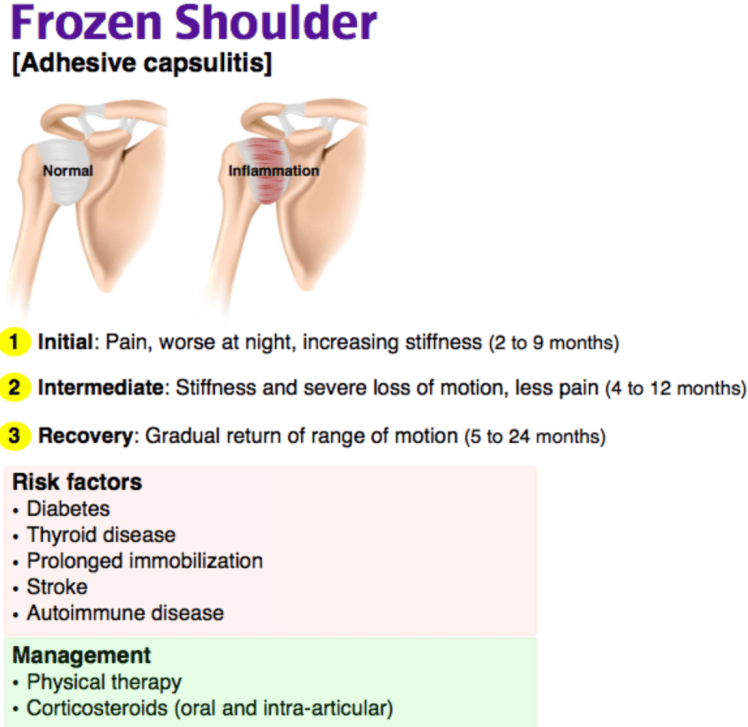
Recurrence risk is directly related to age. Patients under 20 have a >80% recurrence rate. Patients over 40 have higher rates of rotator cuff tear with dislocation — consider outpatient MRI for this group.
Clavicle Fracture Pearls
Middle third fractures (75–80%) are the most common and most benign. Most heal with sling immobilization alone. Lateral third fractures have higher nonunion rates and may need surgical referral. Medial third fractures with posterior displacement are the dangerous ones — they can compress the great vessels, trachea, or esophagus. If you see one, consult orthopedics immediately with thoracic surgery on standby.[3]
Pediatric pearl: If a child with a clavicle fracture is splinting their head to one side, don’t assume it’s just pain — consider getting a cervical spine assessment to rule out atlanto-axial fracture or dislocation.
Proximal Humerus Fracture Pearls
The Neer classification counts displaced parts (>1 cm or >45 degrees angulation). One-part fractures (non-displaced) make up ~80% and are managed conservatively with sling and swathe. Multi-part fractures often need surgery — the goal is surgery within 14 days for displaced fractures, so if outpatient follow-up is unreliable, consider orthopedic consult from the ED.[4]
Recovery is slow. About 90% of recovery occurs in the first 3–4 months, and the remaining 10% takes 6 months or longer. Set expectations at discharge.
AC Separation Grading
Grading is based on the coracoclavicular (CC) distance, not just the AC joint appearance. Types I–II are sprains (ligament stretch/partial tear) — manage with sling, ice, and early motion. Types III and above have complete CC ligament disruption with increasing displacement. Types IV–VI are surgical. Type III is controversial — most are managed conservatively, but high-demand patients may benefit from surgery.[5]
| Type | Finding | Management |
| I | AC ligament sprain, normal X-ray | Sling, early motion |
| II | AC ligament torn, CC intact, mild widening | Sling, early motion |
| III | CC ligament disrupted, 25–100% CC widening | Conservative vs surgical (controversial) |
| IV | Distal clavicle displaced posteriorly into trapezius | Surgical |
| V–VI | Severe superior/inferior displacement | Surgical |
Imaging tip: Consider a CR to visualize both AC joints for comparison. Look at the axillary view for posterior dislocation of the distal clavicle (type IV) — this is missed on AP alone.
Rotator Cuff Pearls
Supraspinatus is involved in the vast majority of tears — it controls the first 30 degrees of abduction. A patient who can’t initiate abduction but can maintain it once passively started likely has a significant supraspinatus tear. The drop-arm test (inability to slowly lower the arm from 90 degrees abduction) is fairly specific for a full-thickness tear.[6]
Acute traumatic tears in younger patients need expedited surgical evaluation — goal is surgeon assessment within 1–2 weeks. Chronic/degenerative tears in older patients can be managed with injection and PT as first-line. Subacromial corticosteroid injection provides relief for up to 3 months and is a reasonable ED intervention for atraumatic rotator cuff pain.
Scapular Fracture Pearls
Scapular fractures require significant force — always look for associated injuries. Pulmonary contusion, rib fractures, pneumothorax, and brachial plexus injuries are common companions. Not all scapular fractures need orthopedic consultation from the ED — body fractures that are non-displaced or minimally comminuted can be managed with sling and outpatient follow-up. Consult for significantly displaced, comminuted, or glenoid-involving fractures.[7]
References
- Hovelius L. Incidence of shoulder dislocation in Sweden. Clin Orthop Relat Res. 1982;166:127-131. PubMed
- Fitch RW, Kuhn JE. Intraarticular lidocaine versus intravenous procedural sedation with narcotics and benzodiazepines for reduction of the dislocated shoulder: a systematic review. Acad Emerg Med. 2008;15(8):703-708. PubMed
- Postacchini F et al. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 2002;11(5):452-456. PubMed
- Neer CS. Displaced proximal humeral fractures: part I. Classification and evaluation. J Bone Joint Surg Am. 1970;52(6):1077-1089. PubMed
- Rockwood CA. Injuries to the acromioclavicular joint. In: Fractures in Adults. 1984. Chapter on AC classification and management.
- Jain NB et al. Clinical examination of the rotator cuff. PM R. 2013;5(1):45-56. PubMed
- Tadros AM et al. Scapula fractures: a review of the literature. Injury. 2009;40(1):46-48. PubMed
