Last reviewed: March 2026
Contents
MDM Templates
Traumatic Hyphema
Patient presents with eye pain and decreased visual acuity after blunt trauma to the eye/face. Slit lamp demonstrates blood layering in the anterior chamber (hyphema). Midface is stable without dental trauma. Negative Seidel sign. IOP within acceptable range. EOM intact without entrapment.
Presentation most consistent with traumatic hyphema. Given traumatic vision loss I have also considered globe rupture, corneal abrasion/ulcer, lens dislocation, retinal detachment, iritis, and orbital fracture with entrapment. No evidence of Le Fort fracture.
Plan: Analgesia and antiemetics. Rigid eye shield placed. Head of bed elevated 30–45 degrees.
If IOP elevated: Timolol 0.5% 1 drop to affected eye.
Ophthalmology consulted regarding hyphema grade, IOP management, cycloplegic initiation, and follow-up interval.
Disposition: Per ophthalmology. Small hyphema (<50%) with normal IOP may be discharged with next-day follow-up. Large hyphema (>50%) or elevated IOP typically requires admission.

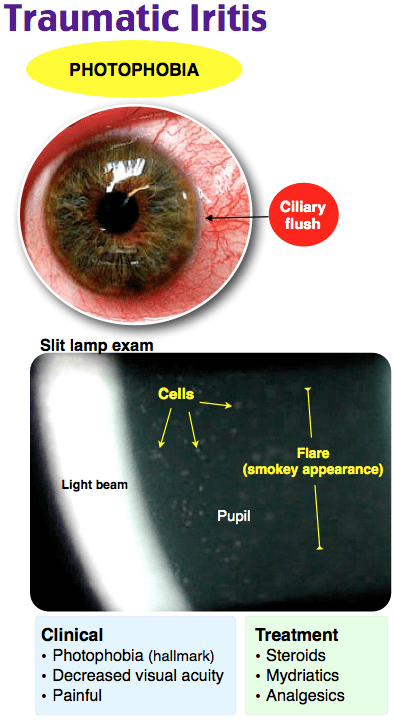
Traumatic Iritis
Patient presents with eye pain and photophobia after blunt ocular trauma. Slit lamp demonstrates ciliary flush, consensual photophobia, and cells/flare in the anterior chamber. No hyphema, no hypopyon. Negative Seidel sign. IOP normal. Visual acuity mildly reduced.
Presentation most consistent with traumatic iritis. History and exam reassure against globe rupture, hyphema, lens dislocation, and corneal abrasion.
Plan: Cycloplegic for pain (homatropine 2% 1 drop TID). Ophthalmology consulted regarding topical steroid initiation.
Disposition: Discharge with ophthalmology follow-up in 24–48 hours. Return precautions for worsening pain, vision loss, or new floaters.
Chemical / Caustic Ocular Injury
Patient presents after chemical exposure to the eye with ***. Pre-irrigation pH: ***. Immediate copious irrigation performed with topical anesthetic. Post-irrigation pH: 7.0–7.2 confirmed on repeat testing at 10 minutes.
Priority was immediate irrigation — do not delay for history or exam. Given the exposure, I have considered corneal epithelial damage, stromal burn, limbal stem cell injury, and risk of secondary glaucoma.
Plan: Proparacaine for analgesia. Irrigation with at least 2 L through Morgan lens until pH normalizes (7.0–7.2) and remains stable on recheck. Fluorescein exam post-irrigation to assess corneal damage. Erythromycin ointment QID. Artificial tears for comfort.
Ophthalmology consulted regarding degree of injury, need for cycloplegic, topical steroid, and follow-up interval.
Disposition: Discharge with ophthalmology follow-up within 24 hours. Return precautions for worsening pain, vision changes, or inability to open the eye.
Clinical Education
Approach to Traumatic Eye Pain
The first priority in any eye trauma is to rule out globe rupture and chemical exposure. If chemical exposure: irrigate immediately — do not pause for visual acuity, slit lamp, or history. If globe rupture suspected (mechanism, teardrop pupil, shallow anterior chamber, Seidel sign): place a rigid eye shield, stop all examination, keep the patient NPO, give antiemetics (vomiting raises IOP), and call ophthalmology emergently.[1]
Hyphema Pearls
Hyphema grading determines management urgency: Grade I: <1/3 anterior chamber. Grade II: 1/3–1/2. Grade III: >1/2. Grade IV: total (“8-ball” hyphema — entire anterior chamber filled with dark blood). Grades III–IV require emergent ophthalmology evaluation for surgical washout risk.[2]
Rebleeding is the major complication — occurs in 5–38% of cases, typically at days 3–5 when the initial clot lyses. Avoid aspirin and NSAIDs (platelet inhibition). Aminocaproic acid (Amicar) may be prescribed by ophthalmology to prevent clot lysis. Bed rest with head elevation at 30–45 degrees allows blood to layer inferiorly and away from the visual axis.[2]
Sickle cell patients with hyphema are high risk — even small hyphemas can cause dangerous IOP elevation because sickled RBCs obstruct the trabecular meshwork. Avoid carbonic anhydrase inhibitors (acetazolamide) in these patients — they acidify the aqueous humor and promote sickling. Timolol is safe. Low threshold for admission and ophthalmology involvement.[2]
Traumatic Iritis Pearls
Traumatic iritis can present days after the initial injury. Patients may return after being seen for a seemingly minor eye injury, now with worsening photophobia. Consensual photophobia (pain in the injured eye when light is shone in the contralateral eye) is the key exam finding. Cells and flare on slit lamp confirm the diagnosis.[3]
Treatment is cycloplegics for pain relief, not mydriatics alone. Homatropine and cyclopentolate paralyze the ciliary muscle (relieving spasm) and prevent posterior synechiae. Topical steroids (prednisolone acetate 1%) are the definitive treatment but should be initiated in consultation with ophthalmology to avoid steroid use in the setting of undiagnosed HSV.
Chemical Injury Pearls
Alkali burns are worse than acid burns. Alkali (lye, cement, drain cleaner, ammonia) causes liquefactive necrosis — it penetrates deeper and continues to damage tissue. Acid causes coagulative necrosis which somewhat limits penetration. Both require aggressive irrigation, but alkali injuries carry a worse prognosis.[4]
Irrigation technique: instill topical anesthetic first (proparacaine). Use a Morgan lens connected to IV tubing running normal saline or LR at a wide-open rate. Irrigate for a minimum of 30 minutes for alkali, 15–20 minutes for acid. Recheck pH 10 minutes after stopping irrigation — if not 7.0–7.2, resume. Evert the lids and sweep the fornices to remove retained particulate matter (especially with cement or plaster).[4]
A white, ischemic-appearing eye after chemical burn is worse than a red one — it indicates limbal ischemia and carries a poor prognosis for corneal healing.
Globe Rupture Red Flags
Stop the exam if you suspect globe rupture. Clues: mechanism (high-velocity projectile, hammering metal on metal), irregular pupil (teardrop pointing toward the wound), shallow anterior chamber, exposed uveal tissue (dark tissue protruding), positive Seidel sign, severely decreased visual acuity, and relative hypotony. Place a rigid eye shield (not a pressure patch), give IV antiemetics, keep NPO, start IV antibiotics (fluoroquinolone), and call ophthalmology emergently. CT orbit is indicated to evaluate for intraocular foreign body.[1]
Disposition
Small hyphema with normal IOP: discharge with ophthalmology next-day follow-up, strict activity restriction. Large hyphema, elevated IOP, or sickle cell: admission. Traumatic iritis: discharge with ophthalmology in 24–48 hours. Chemical injury: discharge after pH normalized with ophthalmology in 24 hours. Globe rupture: emergent ophthalmology for surgical repair.[1]
References
- Sharma R, Brunette DD. Ophthalmology. In: Tintinalli’s Emergency Medicine, 9th ed. McGraw-Hill; 2020.
- Brandt MT, Haug RH. Traumatic hyphema: a comprehensive review. J Oral Maxillofac Surg. 2001;59(12):1462-1470. PubMed
- Rosenbaum JT. Uveitis: etiology, clinical manifestations, and diagnosis. UpToDate. 2024.
- Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and therapy. Surv Ophthalmol. 1997;41(4):275-313. PubMed
