Last reviewed: March 2026
MDM Templates
Uncomplicated Cystitis — Female Discharge
Patient presents with dysuria and urinary frequency. UA supports UTI. Well appearing without systemic infectious signs. Not pregnant. History and exam lower suspicion for pyelonephritis, complicated UTI, STI, ovarian torsion, appendicitis, or other acute abdomen. Plan: Nitrofurantoin 100 mg BID for 5 days. Disposition: Discharge with PCP follow-up if not improving in 48–72 hours. Return for fever, flank pain, vomiting, or worsening symptoms.
Male UTI — Discharge
Patient presents with dysuria. UA supports UTI. No evidence of epididymo-orchitis, prostatitis, deep space GU infection, or STI on exam. Plan: Ciprofloxacin 500 mg BID for 7–14 days (longer course in men due to prostate penetration). Urine gonorrhea/chlamydia sent. Disposition: Discharge with PCP follow-up within 48–72 hours. Return for fever, worsening symptoms, or testicular pain.
Pyelonephritis — Discharge
Patient presents with flank pain, fever, and UA consistent with pyelonephritis. Well appearing, tolerating PO, no complicating factors. Plan: Ciprofloxacin 500 mg BID × 7 days (or ceftriaxone 1 g IV in ED followed by oral step-down). Disposition: Discharge with close PCP follow-up within 24–48 hours. Return for intractable vomiting, worsening, or failure to improve in 48 hours.
Pyelonephritis — Admit
Patient presents with pyelonephritis and *** (unable to tolerate PO/hemodynamic instability/immunocompromised/pregnancy/solitary kidney/concern for obstruction). Plan: IV antibiotics (ceftriaxone 2 g or ciprofloxacin 400 mg IV). Renal imaging to rule out abscess or obstruction. Disposition: Admit for IV antibiotics and monitoring.
ESBL UTI — Cystitis Discharge
Patient with history of ESBL UTI presents with cystitis. No systemic infectious signs. Plan: Nitrofurantoin 100 mg BID × 5 days or fosfomycin 3 g single dose. Urine culture sent for susceptibility. Disposition: Discharge with close follow-up for culture results. Return for fever or worsening.
ESBL UTI — Pyelonephritis Admit
Patient with ESBL history presents with pyelonephritis. Given resistance pattern, oral agents unreliable for upper tract disease. Plan: IV meropenem. Disposition: Admit for IV antibiotics with de-escalation per culture sensitivities.
Procedure Notes
No procedures specific to uncomplicated UTI in the ED. Renal imaging (ultrasound or CT) indicated if concern for abscess, obstruction, or pyelonephritis in high-risk patients.
Clinical Education
Antibiotic Selection for Uncomplicated Cystitis
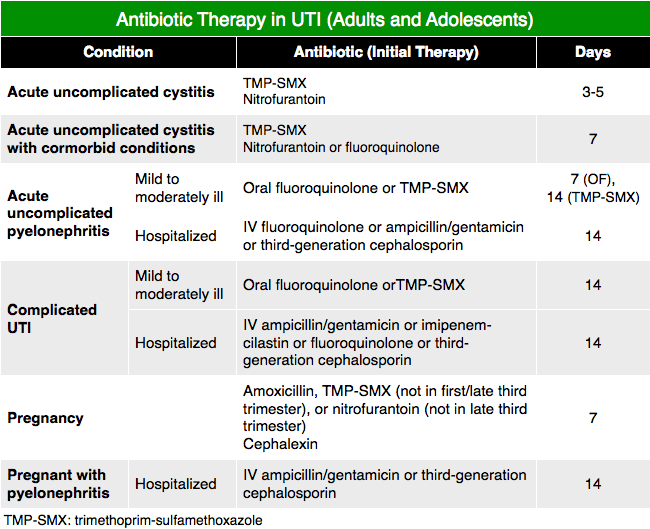
First-line agents per IDSA guidelines: Nitrofurantoin 100 mg BID for 5 days and trimethoprim-sulfamethoxazole DS BID for 3 days are preferred agents in communities with <20% resistance[1]. Fluoroquinolones should be reserved for complicated UTI or pyelonephritis due to concerns about resistance and adverse effects. Cephalexin 500 mg BID for 5–7 days is an alternative if first-line agents are contraindicated[1]. Local resistance patterns guide empiric choice; if >20% resistance to TMP-SMX, nitrofurantoin becomes preferred monotherapy.
Male UTI Considerations
All UTIs in men are considered complicated due to anatomic factors and higher likelihood of prostatitis or upper tract involvement[2]. Longer antibiotic courses (7–14 days) are recommended to ensure adequate prostate penetration. In sexually active men, urine gonorrhea and chlamydia testing should be sent given the overlap in presentation and risk factors. A low WBC count with bacteriuria may suggest STI rather than bacterial UTI and should prompt GC/CT testing[2]. Urinalysis findings may be nonspecific; clinical context and urine culture are essential.
Pyelonephritis Admission Criteria
Admit patients with pyelonephritis if: Age >60 years, pregnant, solitary kidney, immunocompromised (diabetes, malignancy, immunosuppression), unable to tolerate oral intake due to vomiting, concern for obstruction or perinephric abscess, or recent hospitalization/instrumentation[3]. Well-appearing, hemodynamically stable patients without these risk factors may be discharged on oral fluoroquinolones with close outpatient follow-up. Renal ultrasound or CT should be obtained if obstruction is suspected clinically.
ESBL UTI Management
ESBL-producing organisms are resistant to penicillins and cephalosporins. For cystitis, fosfomycin 3 g single dose or nitrofurantoin (which often remains susceptible) are preferred outpatient options[4]. Piperacillin-tazobactam should be avoided as MERINO trial data showed worse outcomes with this agent in ESBL infections; meropenem is the standard for admitted patients requiring IV therapy. Urine culture and susceptibility testing are essential to guide outpatient therapy and ensure appropriate de-escalation.
UTI in Pregnancy
Asymptomatic bacteriuria occurs in 4–7% of pregnant women and must be treated to prevent pyelonephritis. Nitrofurantoin is safe in the first and second trimesters but should be avoided near term due to hemolytic anemia risk[1]. Cephalexin is safe throughout pregnancy. Trimethoprim-sulfamethoxazole should be avoided in the first trimester (folate antagonism) and near term (hyperbilirubinemia risk). A test of cure (repeat UA/culture 1–2 weeks after treatment completion) is required for all pregnant women treated for bacteriuria.
Pediatric UTI Pearls
In children ages 2 months to 2 years with first-time UTI, further imaging with renal ultrasound and voiding cystourethrography is recommended to screen for anatomic abnormalities and vesicoureteral reflux, as these findings alter long-term management. Fever is a common presenting sign and may be the only indication for urinalysis in infants. Suprapubic aspiration or in-and-out catheterization should be used for urine collection in non-toilet-trained children to avoid contamination. Urine bag collection is not reliable for diagnosis in this population.
Urinalysis Interpretation
WBC >5 per high power field with compatible symptoms is diagnostic for UTI; culture confirmation is ideal but not required for diagnosis[5]. Leukocyte esterase has high specificity but low sensitivity and may be negative in early infection. Nitrite is very specific for gram-negative bacteria but misses enterococcus and Pseudomonas. False negative urinalysis can occur with dilute urine, obstruction, or early infection before pyuria develops. Crystalluria (struvite, triple phosphate) may indicate infection with urease-producing organisms; calcium oxalate does not indicate infection.
References
- Infectious Diseases Society of America. Uncomplicated urinary tract infection in women. Clin Infect Dis. 2019;68(7):e16–e50.
- Lipsky BA. Prostatitis and urinary tract infection in men: What’s new; what’s true? Am J Med. 1999;106(3):327–334.
- Gupta K, et al. Infectious Diseases Society of America guidelines for the diagnosis and treatment of asymptomatic bacteriuria in adults. Clin Infect Dis. 2019;68(7):e83–e110.
- Pitout JDD, Laupland KB. Extended-spectrum beta-lactamase-producing Enterobacteriaceae: epidemiology, detection, and treatment. Infect Dis Clin North Am. 2016;30(1):37–52.
- Stamm WE. Diagnosis of urinary tract infection: lessons from research. Infect Dis Clin North Am. 1997;11(4):737–749.
- Smaill F, Vazquez JC. Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane Database Syst Rev. 2019;11:CD000490.

What does SRP mean??
LikeLike
Strict Return Precautions. Better not to abbreviate though.
LikeLike