Last reviewed: March 2026
MDM Templates
Threatened Abortion — Discharge
Patient at *** weeks EGA presents with vaginal bleeding. Ultrasound confirms intrauterine pregnancy with fetal cardiac activity. Cervical os closed. Hemodynamically stable. Rh status checked — RhoGAM administered if Rh-negative. History and exam lower suspicion for ectopic pregnancy, molar pregnancy, or other emergent cause. Plan: Expectant management with pelvic rest. Disposition: Discharge with OBGYN follow-up within 48–72 hours. Return for heavy bleeding, passage of tissue, fever, or severe pain.
Inevitable/Incomplete Abortion
Patient presents with vaginal bleeding, open cervical os, and ultrasound showing ***. Hemodynamically stable. Rh status checked. OBGYN consulted regarding management options: expectant management, medical (misoprostol), or surgical (D&C). Disposition: Per OBGYN — discharge if stable and reliable with close follow-up, or admit for intervention.
Ectopic Pregnancy — Stable
Patient presents with abdominal pain and vaginal bleeding. bHCG *** above discriminatory zone with no intrauterine pregnancy on transvaginal ultrasound. Hemodynamically stable. Presentation concerning for ectopic pregnancy. OBGYN consulted. Plan: If meets methotrexate criteria (unruptured, <4 cm, no fetal cardiac activity, bHCG <5000, able to follow up) — discuss medical vs surgical management with OBGYN. Disposition: Per OBGYN recommendation.
Ectopic Pregnancy — Ruptured/Unstable
Patient presents with abdominal pain, vaginal bleeding, and hemodynamic instability. Free fluid on bedside ultrasound. Presentation consistent with ruptured ectopic pregnancy — a surgical emergency. Plan: Large-bore IV access, type and crossmatch, activate massive transfusion if needed. OBGYN consulted emergently for operative management. Disposition: Emergent OR.
Pregnancy of Unknown Location
Patient presents with vaginal bleeding and positive bHCG (*** mIU/mL) below discriminatory zone. No IUP or ectopic visualized on transvaginal ultrasound. Cannot distinguish between early viable IUP, completed miscarriage, or early ectopic at this time. Rh status checked. Plan: Serial bHCG in 48 hours — should rise >35% if viable IUP, plateau/slow rise concerning for ectopic. Disposition: Discharge with OBGYN follow-up for repeat bHCG in 48 hours. Strict ectopic precautions — return immediately for severe pain, heavy bleeding, or lightheadedness.
Clinical Education
Early Pregnancy Loss Classification
First trimester pregnancy loss is classified by cervical os status and ultrasound findings: Threatened abortion has a closed os with intrauterine pregnancy present; inevitable abortion has an open os with pregnancy in uterus; incomplete abortion has passed products with open os but some tissue remains in uterus; missed abortion (or early fetal demise) has a closed os and no cardiac activity when one was previously documented or should be present by dates; complete abortion shows empty uterus with no gestational sac[1]. Expectant management (awaiting spontaneous passage) is appropriate for threatened, incomplete, and missed abortions if hemodynamically stable and Rh status managed. Medical management with misoprostol or surgical D&C are alternatives discussed with the patient and OBGYN.
Ectopic Pregnancy Recognition
A positive bHCG with no intrauterine pregnancy (IUP) on high-quality transvaginal ultrasound (TVUS) is ectopic pregnancy until proven otherwise. Approximately 2% of all clinically recognized pregnancies are ectopic, and ectopic pregnancy remains the leading cause of first-trimester maternal death in the United States[2]. Risk factors include prior ectopic, pelvic inflammatory disease, IUD use, endometriosis, and assisted reproductive technology. Clinical presentation is highly variable, ranging from asymptomatic (found incidentally) to dramatic hemodynamic collapse with rupture; absence of pain or minimal bleeding does not exclude ectopic pregnancy.
bHCG Interpretation and Discriminatory Zone
The discriminatory zone is the bHCG threshold above which an intrauterine gestational sac should be visible on TVUS; this threshold is typically 1500–2000 mIU/mL on TVUS and 5000–6000 mIU/mL on transabdominal ultrasound[3]. A bHCG above the discriminatory zone with no IUP on TVUS is consistent with ectopic pregnancy. bHCG doubling time in early normal pregnancy is approximately 48 hours; slower rises (48-hour increase <35–50%) are concerning for ectopic pregnancy or nonviable intrauterine pregnancy. Serial bHCG 48 hours apart is essential for patients with findings below discriminatory zone when ultrasound is inconclusive (pregnancy of unknown location).
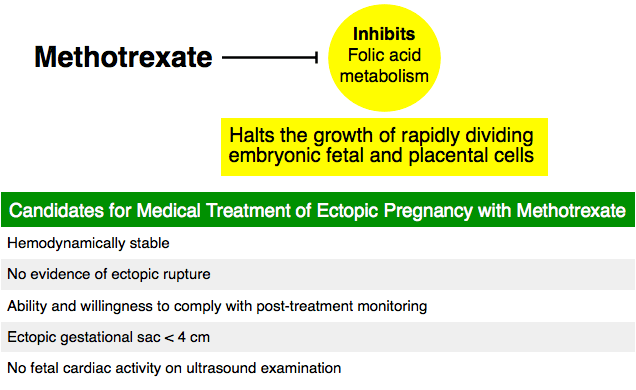
Methotrexate for Ectopic Pregnancy
Methotrexate is a first-line medical treatment for hemodynamically stable unruptured ectopic pregnancy meeting strict criteria. Inclusion criteria are: unruptured ectopic pregnancy, hemodynamic stability, bHCG <5000 mIU/mL, ectopic mass <4 cm on ultrasound, no fetal cardiac activity, no contraindications to methotrexate (hepatic or renal disease, bone marrow suppression, active pulmonary disease), and patient reliability for follow-up[4]. The standard dose is methotrexate 50 mg/m² IM as a single injection. bHCG is monitored at days 4 and 7; a minimum decline of 15% between days 4 and 7 indicates treatment success. Patients unable to comply with serial bHCG monitoring or those with bHCG ≥5000 are managed surgically.
RhoGAM Administration in First Trimester
All Rh-negative, non-sensitized women with first-trimester vaginal bleeding or pregnancy loss require RhoGAM to prevent alloimmunization. The dose for bleeding before 12 weeks is 50 mcg IM; for bleeding after 12 weeks, 300 mcg IM is given[5]. RhoGAM should be administered within 72 hours of the bleeding event but may be given up to 28 days with diminishing efficacy. Confirmation of Rh-negative status and negative antibody screen should be documented before administration. Rh-positive and already sensitized patients do not require RhoGAM but should be counseled about risks.
Ultrasound Landmarks by Gestational Age
Transvaginal ultrasound findings correlate closely with gestational age in early pregnancy: The gestational sac is first visualized at approximately 5 weeks EGA (bHCG ~1000 mIU/mL) as an echogenic ring; a yolk sac appears by 5.5 weeks indicating an intrauterine (not pseudosac) pregnancy; a fetal pole is visible by 6 weeks; and cardiac activity is typically seen by 6–6.5 weeks[3]. Absence of expected structures at these thresholds raises concern for dating error, nonviable pregnancy, or ectopic pregnancy. Mean gestational sac diameter (MSD) growth of >3 mm between two ultrasounds is reassuring; slow growth suggests nonviable intrauterine pregnancy.
Septic Abortion
Septic abortion (fever + vaginal bleeding + uterine tenderness ± recent instrumentation/illegal abortion) is a medical emergency. Blood cultures should be drawn and broad-spectrum antibiotics initiated immediately without awaiting culture results; typical organisms include gram-negative rods, anaerobes, and streptococci. Imaging (ultrasound or CT) is obtained to assess for retained products of conception, perforation, or abscess. OBGYN consultation for emergent D&C is necessary; do not delay antibiotics or operative management while awaiting diagnostic studies[1]. Disseminated intravascular coagulation, septic shock, and acute kidney injury are potential complications requiring ICU-level care.
References
- Creinin MD, Harwood B, Guido RS. Diagnosis and management of early pregnancy loss. Obstet Gynecol. 2019;134(1):e1–e12.
- Bouyer J, et al. Ectopic pregnancy and increased overall and cardiovascular mortality risk. Fertil Steril. 2012;97(1):44–51.
- Barnhart KT. Clinical practice. Ectopic pregnancy. N Engl J Med. 2005;353(25):2701–2708.
- Lipscomb GH, et al. Nonsurgical treatment of ectopic pregnancy. N Engl J Med. 1999;340(5):287–291.
- American College of Obstetricians and Gynecologists. Prevention of Rh D alloimmunization. ACOG Practice Bulletin. 2017;(181).
- Doubilet PM, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369(15):1443–1451.
