Last reviewed: March 2026
Contents
MDM Templates
Bacterial Meningitis (Suspected)
Patient presents with headache, fever, and neck stiffness. Exam notable for meningismus. No focal neurologic deficits, no papilledema.
Presentation concerning for bacterial meningitis. Empiric antibiotics administered prior to LP — do not delay antibiotics for imaging or LP. Not consistent with viral meningitis alone given degree of toxicity, though CSF results will help differentiate. Subarachnoid hemorrhage also considered but fever and meningismus point toward infection.
If CT required before LP (immunocompromised, focal deficits, seizure, papilledema, or significantly altered): Blood cultures drawn and empiric antibiotics given before CT. LP performed after CT if no contraindication.
Plan: Empiric antibiotics initiated. LP performed. Blood cultures obtained. Neurology and/or infectious disease consulted. Admit.
Viral / Aseptic Meningitis
Patient presents with headache, photophobia, and low-grade fever. Exam notable for mild neck stiffness. Well appearing. No focal neurologic deficits, no altered mentation.
CSF profile consistent with viral meningitis — lymphocytic pleocytosis, normal glucose, mildly elevated protein, negative gram stain. Presentation and CSF not consistent with bacterial meningitis. No behavioral changes, no focal deficits, and no temporal lobe findings to suggest HSV encephalitis.
If still symptomatic or unable to confirm viral pattern: Admit on empiric antibiotics until cultures finalize at 48 hours.
Plan: Discharge with close PCP follow-up within 24 hours. Return for worsening headache, high fevers, confusion, neck stiffness, or new neurologic symptoms.
Clinical Education
Approach to Suspected Meningitis
Don’t delay antibiotics. The single most important action in suspected bacterial meningitis is giving antibiotics immediately. Every hour of delay increases mortality. If you need a CT before LP, give antibiotics first, then image, then LP. A partially treated LP is better than a dead patient with a pristine CSF sample.[1]
The classic triad (fever, neck stiffness, altered mentation) is present in only ~45% of cases. Two of three are present in ~95%. A completely well-appearing, afebrile patient with a normal exam is extremely unlikely to have bacterial meningitis. But if any two of the triad are present, you should LP.[2]
Kernig and Brudzinski signs have terrible sensitivity (~5% each). Their absence means nothing. A supple neck in an ill-appearing febrile patient does not rule out meningitis.
CT Before LP
Most patients do not need CT before LP. Per Hasbun et al. (NEJM 2001), LP without preceding CT is safe if all of the following are true: age <60, not immunocompromised, no history of CNS disease, no seizure within 1 week, normal level of consciousness, and no focal neurologic deficits. If none of these are present, the chance of a normal CT is 97% and no patients herniated.[3]
If CT is indicated, give antibiotics and dexamethasone BEFORE CT. Do not let imaging delay treatment. Draw blood cultures, give antibiotics, get CT, then LP.
CSF Interpretation
| Parameter | Bacterial | Viral | TB / Fungal |
| WBC | >1,000 (often >5,000) | 10–500 | 100–500 |
| Predominant cell | PMNs (>80%) | Lymphocytes | Lymphocytes |
| Glucose | Low (<40 or ratio <0.4) | Normal | Low |
| Protein | High (>250) | Mildly elevated | High |
| Gram stain | Positive in ~60–80% | Negative | AFB rarely positive |
Early viral meningitis can have PMN predominance. In the first 24 hours, viral CSF may show >50% PMNs, mimicking bacterial. If the glucose is normal and the patient looks nontoxic, consider repeating LP in 12–24 hours or admitting on empiric antibiotics until cultures return.[1]
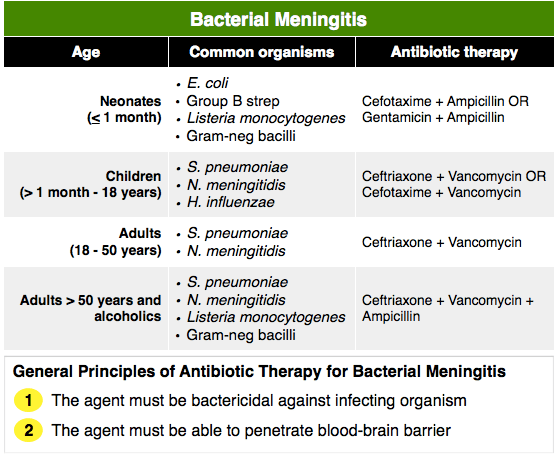
Empiric Antibiotic Regimens
| Population | Regimen | Rationale |
| Adult <50, immunocompetent | Ceftriaxone 2g IV + Vancomycin 15–20 mg/kg IV | Covers S. pneumoniae (including resistant) + N. meningitidis |
| Adult ≥50 or immunocompromised | Ceftriaxone 2g IV + Vancomycin 15–20 mg/kg IV + Ampicillin 2g IV | Add Ampicillin for Listeria coverage |
| Neonate (<1 month) | Ampicillin + Gentamicin (or Cefotaxime) | GBS, E. coli, Listeria |
Add dexamethasone 0.15 mg/kg IV before or with the first dose of antibiotics in suspected bacterial meningitis. Most beneficial for pneumococcal meningitis — reduces mortality and hearing loss. Must be given before or with antibiotics to have benefit; giving it after antibiotics is too late.[4]
HSV Encephalitis
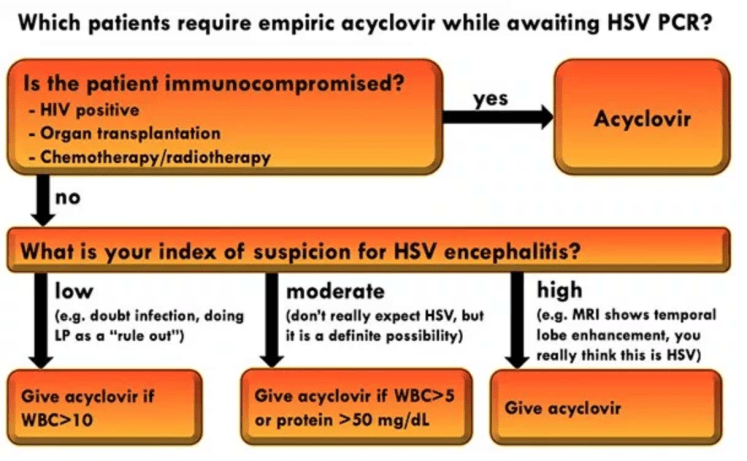
Consider HSV encephalitis in any patient with viral meningitis plus altered mentation, behavioral changes, seizures, or focal neurologic deficits — particularly temporal lobe signs. HSV encephalitis is the one viral CNS infection that is treatable and fatal if missed. Add acyclovir 10 mg/kg IV if there is any suspicion.[5]
MRI is more sensitive than CT for temporal lobe changes. CSF HSV PCR is the definitive test but takes time to result. Don’t wait for the PCR to start acyclovir.
Chemoprophylaxis for Contacts
Only required for N. meningitidis (meningococcal meningitis). Close contacts (household members, anyone with direct exposure to oral secretions) need prophylaxis. Options: rifampin 600 mg PO BID x 2 days, ciprofloxacin 500 mg PO x 1 dose, or ceftriaxone 250 mg IM x 1 dose. Ceftriaxone is preferred for pregnant contacts.
Healthcare workers only need prophylaxis if they performed unprotected mouth-to-mouth or unprotected intubation. Routine patient care with standard precautions does not require prophylaxis.
Disposition
Admit all suspected bacterial meningitis on empiric antibiotics with cultures pending. These patients need close monitoring for complications including seizures, cerebral edema, and septic shock.
Viral meningitis can be discharged if the patient is well appearing, can tolerate oral fluids, has reliable follow-up within 24 hours, and you are confident in the viral CSF profile. If there is any diagnostic uncertainty, admit on empiric antibiotics until cultures finalize at 48 hours.
HSV encephalitis is an ICU admission. Start acyclovir empirically and do not discharge.
References
- van de Beek D, de Gans J, Tunkel AR, Wijdicks EF. Community-acquired bacterial meningitis in adults. N Engl J Med. 2006;354(1):44-53. PubMed
- van de Beek D, de Gans J, Spanjaard L, et al. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004;351(18):1849-1859. PubMed
- Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the head before lumbar puncture in adults with suspected meningitis. N Engl J Med. 2001;345(24):1727-1733. PubMed
- de Gans J, van de Beek D. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347(20):1549-1556. PubMed
- Tunkel AR, Glaser CA, Bloch KC, et al. The management of encephalitis: clinical practice guidelines by IDSA. Clin Infect Dis. 2008;47(3):303-327. PubMed
