MDM Templates
Urethritis/Cervicitis — Discharge
Patient presents with dysuria and/or discharge. Exam consistent with urethritis/cervicitis without complications. No epididymo-orchitis, PID, disseminated infection, or deep space infection on exam. Plan: Empiric treatment for gonorrhea and chlamydia — ceftriaxone 500 mg IM plus doxycycline 100 mg BID x 7 days. Disposition: Discharge with partner notification counseling. Follow-up with PCP. Return for worsening symptoms, fever, or rash.
PID — Outpatient
Patient presents with pelvic pain and cervical motion tenderness consistent with pelvic inflammatory disease. No TOA on imaging. Tolerating PO. No peritoneal signs. Plan: Ceftriaxone 500 mg IM plus doxycycline 100 mg BID x 14 days plus metronidazole 500 mg BID x 14 days. Disposition: Discharge with OBGYN follow-up in 48-72 hours. Return for fever, worsening pain, or vomiting.
PID — Admit
Patient presents with PID and *** (TOA/peritoneal signs/unable to tolerate PO/failed outpatient therapy/pregnancy). Plan: IV cefoxitin plus doxycycline (or clindamycin plus gentamicin). OBGYN consulted. Disposition: Admit for IV antibiotics and monitoring.
Genital Ulcer — HSV
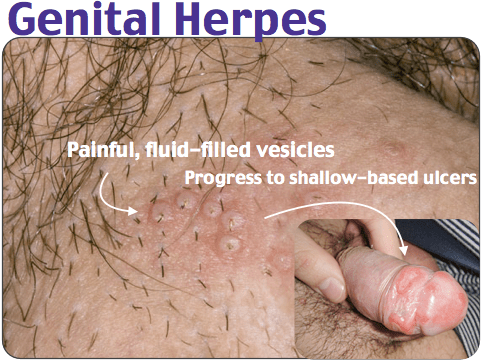
Patient presents with painful genital ulcers consistent with primary herpes simplex. No secondary syphilis features, no disseminated infection. Plan: Valacyclovir 1 g BID x 7-10 days (primary outbreak). Disposition: Discharge with PCP/ID follow-up for long-term management and partner counseling.
Disseminated Gonococcal Infection
Patient presents with migratory polyarthralgia, tenosynovitis, and pustular skin lesions concerning for disseminated gonococcal infection. Plan: Blood and joint cultures obtained. IV ceftriaxone 1 g daily. ID consulted. Disposition: Admit for IV antibiotics.
Clinical Education
Gonorrhea Treatment Update
Current CDC 2021 guidelines recommend ceftriaxone 500 mg IM as monotherapy. Azithromycin is no longer routinely co-prescribed; doxycycline is added only to cover concurrent chlamydia or if chlamydia has not been excluded by testing. Rising cephalosporin resistance globally has prompted guideline changes and heightened surveillance. Patients should be counseled regarding partner notification, testing for other STIs (chlamydia, syphilis, HIV), and the importance of completing antibiotic courses. Test of cure is no longer routinely performed; instead, reinfection screening at 3 months is recommended for those at high risk[1].
Chlamydia and PID
Untreated chlamydia carries a significant risk of ascending infection and pelvic inflammatory disease. PID substantially increases the risk of ectopic pregnancy, infertility, and chronic pelvic pain. There is a low threshold to treat empirically with appropriate antibiotics in patients presenting with pelvic pain and cervical motion tenderness, even without definitive laboratory confirmation, because the morbidity of delayed treatment outweighs the risks of empiric therapy. Doxycycline 100 mg BID for 7 days is effective treatment for uncomplicated chlamydia; for PID, longer duration (14 days) with the addition of metronidazole is standard. All sexual partners should be notified and treated[2].
Genital Ulcer Differential
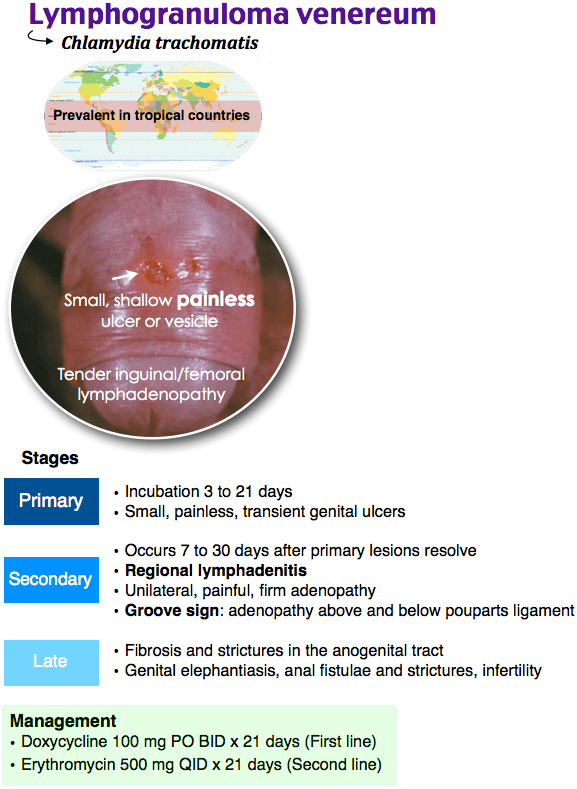
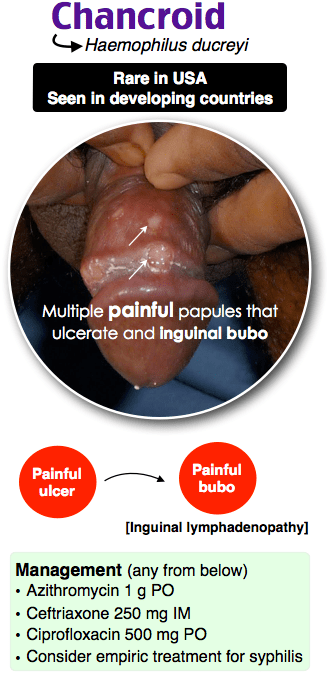
The character and associated symptoms of genital ulcers help narrow the differential diagnosis. Painful ulcers typically suggest herpes simplex or chancroid, whereas painless or minimally painful ulcers suggest syphilis (primary chancre) or lymphogranuloma venereum (LGV). Herpes typically presents with vesicles that progress to painful ulcers; chancroid (caused by Haemophilus ducreyi) is rare in the United States but presents with deep, purulent painful ulcers. The following table summarizes key features:
| Condition | Pain | Appearance | Key Features |
|---|---|---|---|
| Herpes Simplex | Painful | Vesicles, shallow ulcers | Prodrome, rapid onset, HSV PCR/culture |
| Chancroid | Painful | Deep, purulent ulcer | Painful adenopathy, rare in US |
| Syphilis (Primary) | Painless/minimal | Indurated chancre, clean base | Painless adenopathy, RPR/VDRL+ |
| LGV | Painless/minimal | Small papule or shallow ulcer | Severe painful inguinal adenopathy |
Testing should include herpes PCR, syphilis serology (RPR/VDRL with confirmatory TPPA/FTA-ABS), and in at-risk patients, LGV testing (Chlamydia trachomatis L1/L2/L3 by nucleic acid amplification)[3].
Syphilis Stages and Treatment
Syphilis progresses through distinct clinical stages, each with specific diagnostic and treatment considerations. Primary syphilis presents with an indurated chancre at the site of inoculation; secondary syphilis (weeks to months after primary) is characterized by a systemic rash, mucous patches, condyloma lata, generalized lymphadenopathy, and constitutional symptoms. Tertiary syphilis (years later) includes neurosyphilis, cardiovascular disease, and gummatous lesions. All stages should be treated with benzathine penicillin G 2.4 million units IM (1.2M in each buttock) as a single dose for primary and secondary disease. Patients should be warned of the Jarisch-Herxheimer reaction — an acute febrile response occurring 12-24 hours after the first dose — which, while usually self-limited, can be severe. Diagnosis is confirmed by non-treponemal testing (RPR/VDRL) with subsequent treponemal confirmation (TPPA, FTA-ABS, or TP-PA)[4].
HIV PEP and PrEP
Post-exposure prophylaxis (PEP) must be initiated within 72 hours of a potential HIV exposure to be effective. Current regimens typically consist of 28 days of combination antiretroviral therapy (e.g., tenofovir-emtricitabine plus raltegravir or dolutegravir). Efficacy decreases substantially if initiated after 72 hours, and guidelines recommend starting as soon as possible. PrEP (pre-exposure prophylaxis) is indicated for high-risk individuals and involves daily or event-based dosing of tenofovir-emtricitabine; it is highly effective (>90%) when adherence is maintained. Both PEP and PrEP initiation often involves infectious disease consultation and baseline HIV testing to confirm negative status prior to starting therapy. Patients initiating PrEP should be counseled regarding adherence, periodic monitoring, and the importance of regular HIV testing[5].
Sexual Assault Prophylaxis Protocol
Emergency providers must be prepared to offer comprehensive STI prophylaxis and other preventive measures to sexual assault survivors. Empiric treatment includes ceftriaxone 500 mg IM (or cefixime 400 mg PO if cephalosporin allergy and low risk for gonorrhea), plus doxycycline 100 mg BID x 7 days (or azithromycin 1 g single dose if doxycycline contraindicated), plus metronidazole 500 mg BID x 7 days to cover trichomonas and anaerobes. Additionally, emergency contraception should be offered if the victim is of childbearing age and within the appropriate window; hepatitis B vaccination (or HBIG if unvaccinated and source unknown); and HIV PEP if risk is assessed as substantial. All patients should be offered sexual assault evidence collection (if presenting within the appropriate window), counseling, and follow-up care with trauma-informed services. Reporting requirements vary by state and should be clarified with local authorities and the patient’s informed consent[6].
Reporting Requirements
Many STIs are reportable to public health authorities, and requirements vary by state and jurisdiction. Gonorrhea, chlamydia, syphilis, and HIV are uniformly reportable in all U.S. states. Some states also require reporting of HSV in certain circumstances or for healthcare worker exposures. Providers should familiarize themselves with their local health department regulations. Reporting is typically made to the local health department and is essential for partner notification, outbreak investigation, and epidemiologic tracking. Patient confidentiality is protected by public health law, and notification of partners (often performed by health department disease investigators) is a critical step in breaking chains of transmission. Prompt and accurate reporting supports community health while respecting individual privacy[1].
References
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187.
- Taylor SN, Marrazzo JM, Batteiger BE, et al. Single-dose cefotaxime for treatment of uncomplicated gonorrhea. Sex Transm Dis. 2009;36(2):89-91.
- Suntoke TR, Wroblewski JK, Mabey DC, et al. Lymphogranuloma venereum: Current perspectives. HIV AIDS (Auckl). 2010;2:39-50.
- Clement ME, Okeke NL, Hicks CB. Treatment of syphilis: A systematic review. JAMA. 2014;312(18):1905-1917.
- Mayer KH, Krakower DS, Hawkins D. Treating and preventing HIV-1 infection: A review. JAMA. 2015;314(2):155-166.
- Holmes MM, Resnick HS, Kilpatrick DG, et al. Rape-related pregnancy: Estimates and descriptive characteristics based on national sample of women. Am J Obstet Gynecol. 1996;175(2):320-325.

Need update: Current recommendations are Rocephin 500mg IM (1000mg if >150kg) and Doxycycine 100mg BID x7 days
LikeLike
Updated, thank you, though good to keep in mind patient compliance and potential benefit of single dose treatment versus relying on prescription filling.
LikeLike