Last reviewed: March 2026
Contents
MDM Templates
Acute Angle-Closure Glaucoma
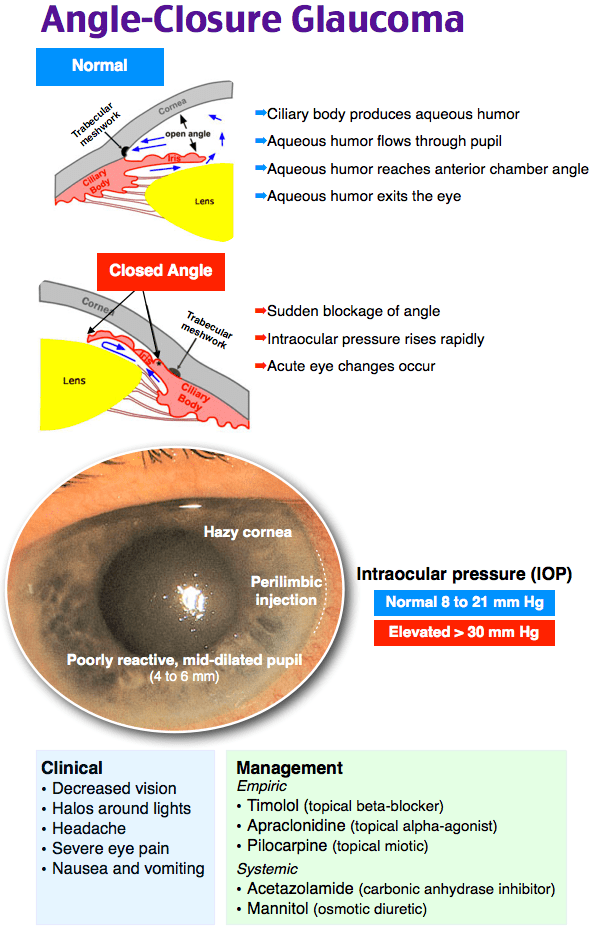
Patient presents with painful unilateral vision loss, headache, and nausea/vomiting. Exam demonstrates a mid-dilated, fixed pupil with conjunctival injection and corneal haze in the affected eye. IOP is significantly elevated.
Presentation most consistent with acute angle-closure glaucoma. Given painful vision loss I have also considered corneal ulcer, uveitis, endophthalmitis, orbital cellulitis, and optic neuritis. No trauma, no foreign body on exam, negative Seidel sign.
Plan: Timolol 0.5% 1 drop to affected eye. Pilocarpine 1–2% 1 drop to affected eye, repeated at 15 minutes. Acetazolamide 500 mg PO. Prednisolone acetate 1% 1 drop to affected eye. Analgesia and antiemetics.
Ophthalmology consulted regarding IOP response, need for additional agents (apraclonidine, mannitol), and disposition. Definitive treatment is laser peripheral iridotomy.
Disposition: Per ophthalmology recommendation. Admit if IOP refractory.
Anterior Uveitis / Iritis
Patient presents with eye pain, photophobia, and decreased visual acuity. Slit lamp demonstrates cells and flare in the anterior chamber. Consensual photophobia present. No hypopyon. No corneal defect on fluorescein.
Presentation most consistent with anterior uveitis. History and exam reassure against corneal ulcer, acute angle-closure glaucoma, endophthalmitis, and optic neuritis.
Plan: Cycloplegic for pain (cyclopentolate 1% TID or homatropine 2% TID). Ophthalmology consulted regarding topical steroid initiation (prednisolone acetate 1%).
Disposition: Discharge with ophthalmology follow-up in 24–48 hours. Return precautions for worsening pain, vision loss, or fever.
Optic Neuritis
Patient presents with subacute unilateral vision loss with pain on eye movement. Exam demonstrates decreased visual acuity, afferent pupillary defect (APD), and dyschromatopsia (impaired color vision). No external eye abnormality. Fundoscopy may show optic disc edema or may be normal (retrobulbar neuritis).
Presentation most concerning for optic neuritis. Given painful vision loss I have also considered acute angle-closure glaucoma, orbital cellulitis, endophthalmitis, and giant cell arteritis. No fever, no proptosis, no conjunctival injection to suggest orbital process.
Plan: MRI brain and orbits with gadolinium and fat suppression.
Ophthalmology and neurology consulted regarding imaging findings, IV methylprednisolone initiation, and disposition.
Disposition: Admit for IV steroids if confirmed. MRI findings guide MS workup and long-term management.
Endophthalmitis
Patient presents with severe eye pain, vision loss, and purulent-appearing eye with conjunctival injection and chemosis. History of recent eye surgery or intravitreal injection ***. Exam demonstrates hypopyon and significant anterior chamber inflammation.
Presentation highly concerning for endophthalmitis. This is an ophthalmologic emergency requiring emergent consultation for intravitreal cultures and antibiotics.
Plan: Emergent ophthalmology consultation.
Ophthalmology consulted regarding intravitreal tap and injection, systemic antibiotics, and disposition.
Disposition: Per ophthalmology — typically requires admission or same-day operative intervention.
Clinical Education
Approach to Painful Vision Loss
Painful vision loss is dangerous until proven otherwise. The differential is shorter than painless vision loss and includes: acute angle-closure glaucoma, corneal pathology (ulcer, keratitis), anterior uveitis/iritis, endophthalmitis, optic neuritis, and orbital cellulitis. A slit lamp exam with IOP measurement and fluorescein staining sorts most of these.[1]
Acute Angle-Closure Glaucoma Pearls
The classic presentation mimics an abdominal emergency. Patients often present with headache, nausea, vomiting, and abdominal pain — the eye complaint may be secondary. Always check pupils and IOP in patients with headache and vomiting. Risk factors: older age, female sex, Asian descent, hyperopia (farsightedness), and shallow anterior chamber.[2]
Treatment ladder: The goal is to decrease aqueous humor production and increase outflow while relieving the pupillary block. Timolol and acetazolamide decrease production. Pilocarpine causes miosis to open the drainage angle — but it may not work initially because ischemic pupillary sphincter paralysis occurs at IOP >40–50 mmHg. Give it anyway upon diagnosis, but expect it to become effective as IOP drops from other agents. Treat pain and nausea aggressively — both can further elevate IOP.[2]
Do not patch the eye — darkness promotes pupillary dilation and worsens the angle closure. Keep the room lit and the patient supine.[2]
Refractory IOP: if IOP remains elevated after 2 rounds of topical agents plus acetazolamide, consider IV mannitol 1–2 g/kg (osmotic diuretic). Contraindicated in CHF and renal failure. Use isosorbide in diabetics (mannitol is metabolized to glucose).[2]
Anterior Uveitis Pearls
Consensual photophobia is the clinical pearl for uveitis. Pain in the affected eye when a penlight is shone in the contralateral eye occurs because the consensual pupillary constriction irritates the inflamed ciliary body. This finding is relatively specific and can be elicited without a slit lamp.[3]
Cycloplegics (not just mydriatics) are the key treatment for pain. They paralyze the ciliary muscle, relieving spasm pain, and prevent posterior synechiae (iris adhesions to the lens). Homatropine and cyclopentolate are preferred over tropicamide because they provide longer-lasting cycloplegia. Topical steroids are the definitive treatment but should be initiated in consultation with ophthalmology.[3]
Recurrent uveitis warrants rheumatologic workup for associated conditions: ankylosing spondylitis, sarcoidosis, Behçet disease, inflammatory bowel disease, reactive arthritis. HLA-B27 is the most commonly associated marker.
Optic Neuritis Pearls
The Optic Neuritis Treatment Trial (ONTT) established the treatment paradigm. IV methylprednisolone (1 g daily for 3 days, then oral taper) speeds visual recovery but does not change long-term visual outcome. Oral prednisone alone was associated with higher recurrence rates and should not be used as monotherapy.[4]
MRI is essential — not just for diagnosis but for prognosis. The presence of white matter lesions on brain MRI predicts conversion to multiple sclerosis. Patients with a normal brain MRI have ~25% risk of MS at 15 years; those with >=1 lesion have ~72% risk.[4]
The triad to remember: (1) pain with eye movement, (2) APD (afferent pupillary defect — the swinging flashlight test), (3) dyschromatopsia (red desaturation). The fundus may look completely normal in retrobulbar neuritis — “the patient sees nothing and the doctor sees nothing.”
Endophthalmitis Pearls
Endophthalmitis is a true ophthalmologic emergency. >90% of cases are exogenous (post-operative, post-injection, post-trauma). Onset is typically 2–7 days after the inciting event. The hallmark finding is hypopyon (layering of pus in the anterior chamber) with severely reduced vision. Do not delay ophthalmology consultation for imaging or labs — the patient needs intravitreal antibiotics (vancomycin + ceftazidime) as soon as possible.[5]
Disposition
Acute angle-closure glaucoma: admit or prolonged ED observation until IOP controlled, with ophthalmology managing disposition. Anterior uveitis: discharge with ophthalmology follow-up in 24–48 hours. Optic neuritis: admit for IV steroids and MRI. Endophthalmitis: emergent ophthalmology consultation and likely operative intervention.[1]
References
- Sharma R, Brunette DD. Ophthalmology. In: Tintinalli’s Emergency Medicine, 9th ed. McGraw-Hill; 2020.
- Prum BE et al. Primary Angle Closure — Preferred Practice Pattern. Ophthalmology. 2016;123(1):P1-P40. PubMed
- Rosenbaum JT. Uveitis: etiology, clinical manifestations, and diagnosis. UpToDate. 2024.
- Beck RW et al. The Optic Neuritis Treatment Trial: three-year follow-up results. Arch Ophthalmol. 1995;113(2):136-137. PubMed
- Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study. Arch Ophthalmol. 1995;113(12):1479-1496. PubMed
