Last reviewed: March 2026Contents
- MDM Templates
- Clinical Education
- Thrombolytic Eligibility & Dosing
- The Evidence Debate: Thrombolytics
- Thrombectomy & Extended Windows
- BP Management in Acute Stroke
- Stroke Syndromes by Vascular Distribution
- Peripheral & Atypical Stroke Presentations
- Wake-Up Stroke & Unknown LKWT
- Stroke Mimics
- Recrudescence
- Scoring Tools: NIHSS & RACE
- References
MDM Templates
Stroke Alert
Patient presents with acute neurologic deficit(s): ***.
Last known well time: ***.
NIHSS: ***.
PMH stroke risk factors include: ***.
Presentation less suspicious for infectious etiology, toxicologic ingestion, post-ictal state, or complex migraine.
History and exam are concerning for acute ischemic stroke. CT head shows no hemorrhagic stroke.
Neurology consultation:
Discussed with Dr. *** (Neurology) regarding patient’s acute neurologic deficits, NIHSS, last known well time, imaging findings, and their potential for thrombolysis. Shared decision that patient *** meets / does not meet criteria for IV thrombolysis.
If large vessel occlusion considered (NIH>6 or cortical signs):
Neurointerventional consultation:
Discussed with Dr. *** (Neurointerventional) the patient’s consideration/potential for thrombectomy.
Patient meets / does not meet criteria for mechanical thrombectomy based on symptoms and clinical-imaging mismatch evaluation.
Disposition: Admission for continuous neuromonitoring, serial neurologic exams, and stroke workup. Stroke neurology following.
Thrombolytic Consent & Administration
Verbal consent to proceed with IV thrombolysis was obtained with nursing at bedside.
Patient displays all four key elements of capacity. They understand that receiving IV thrombolysis for presumed ischemic stroke may improve recovery by dissolving the clot blocking blood flow to the brain and potentially reducing long-term disability. They also understand the treatment carries risks, primarily bleeding — including intracranial hemorrhage in approximately 6–7% of patients — which can worsen disability or be life-threatening.[1]
The risks, benefits, and alternatives — including not receiving thrombolytics — were discussed. The evidence supporting thrombolysis shows modest benefit with a number needed to treat of approximately 10 for meaningful functional improvement, and the patient was informed that the evidence base, while supportive, involves uncertainty.[10]
*** After thorough discussion with nursing at bedside, the patient confirmed they *** (WOULD / WOULD NOT) like to proceed with treatment.
If tenecteplase:
Tenecteplase 0.25 mg/kg IV bolus (max 25 mg) administered at ***. Total dose: *** mg.
If alteplase:
Alteplase 0.9 mg/kg IV (max 90 mg). 10% (*** mg) administered as IV bolus at ***; remainder (*** mg) infusing over 60 minutes.
Post-thrombolytic BP goal: <180/105 for 24 hours. Patient monitored for signs of angioedema, hemorrhage, or neurologic change. Neurology aware.
Clinical Education
Thrombolytic Eligibility & Dosing
Tenecteplase is increasingly preferred over alteplase for acute ischemic stroke. The AcT trial demonstrated non-inferiority of tenecteplase to alteplase with the practical advantage of a single IV bolus rather than a 60-minute infusion.[7] AHA/ASA 2024 updated guidelines now include tenecteplase as a recommended alternative.[11]
| Agent | Dose | Administration |
| Tenecteplase | 0.25 mg/kg IV (max 25 mg) | Single IV bolus over 5 seconds |
| Alteplase | 0.9 mg/kg IV (max 90 mg) | 10% as bolus, remainder over 60 min |
Standard window: Within 4.5 hours of last known well time.[2]
Pre-treatment BP requirement: Must be <185/110 before administration. Treat with labetalol or nicardipine if above threshold and reassess.
Key contraindications (abbreviated): Active internal bleeding, intracranial hemorrhage on CT, recent intracranial/spinal surgery or serious head trauma (3 months), intracranial neoplasm/AVM/aneurysm, known bleeding diathesis, platelet count <100k, INR >1.7 or PT >15s, current anticoagulant use with elevated INR/aPTT, SBP >185 or DBP >110 despite treatment.[8]
Additional exclusions in the 3–4.5 hour window (per ECASS-III criteria): age >80, NIHSS >25, oral anticoagulant use regardless of INR, history of both diabetes AND prior stroke.[2]
Symptomatic ICH risk by age: Under 50: ~1–2%. Age 50–65: ~2–4%. Age 65–75: ~4–6%. Over 75: ~6–10%.[1]
The Evidence Debate: Thrombolytics
The evidence supporting IV thrombolytics for ischemic stroke is more nuanced than commonly taught. This matters at the bedside because shared decision-making requires an honest assessment of both benefit and uncertainty.
NINDS (1995) — the foundational trial — enrolled 624 patients and showed a 12% absolute increase in patients with minimal or no disability at 90 days. However, it has been criticized for a baseline imbalance: the placebo group had more severe strokes at baseline, which may have inflated the treatment effect. The rate of symptomatic ICH was 6.4% in the treatment group vs 0.6% in placebo.[1]
ECASS-III (2008) extended the window to 4.5 hours and showed benefit, but excluded patients >80, those with NIHSS >25, oral anticoagulant users, and those with both diabetes and prior stroke — a significant portion of the real-world stroke population.[2]
IST-3 (2012) was the largest thrombolytic stroke trial (3,035 patients) and was negative on its primary outcome (Oxford Handicap Scale 0–2 at 6 months). Secondary analyses suggested benefit in certain subgroups, but the primary endpoint did not reach significance.[3]
The Emberson meta-analysis (2014) pooled individual patient data from 9 trials and showed that earlier treatment yields greater benefit — NNT ~10 within 3 hours, ~20 at 3–4.5 hours — but acknowledged the consistent ~6% absolute increase in symptomatic ICH.[10]
The skeptic’s perspective (notably Jerry Hoffman on EMRAP) argues: the absolute benefit is modest, the trials had methodological concerns (particularly NINDS baseline imbalance), the harm of ICH is real and iatrogenic, and most patients overestimate the benefit during consent discussions. The takeaway is not that thrombolytics should never be given, but that the conversation with patients should include genuine uncertainty rather than presenting treatment as clearly beneficial.[9]
Bottom line for the ED: Thrombolytics remain guideline-recommended, and most stroke neurologists strongly support their use. But an informed consent discussion should include that roughly 1 in 10 patients meaningfully benefits, roughly 1 in 15–20 has symptomatic ICH, and the evidence base — while supportive overall — has legitimate criticisms. Time matters: the earlier, the better the risk-benefit ratio.
Thrombectomy & Extended Windows
Mechanical thrombectomy for large vessel occlusion (LVO) has stronger evidence and larger effect sizes than IV thrombolytics. Multiple landmark trials (MR CLEAN, ESCAPE, EXTEND-IA, SWIFT PRIME, REVASCAT) demonstrated clear benefit within 6 hours.[8]
DAWN trial (2018): Thrombectomy at 6–24 hours in patients with clinical-imaging mismatch (significant deficit but small infarct core on perfusion imaging). The NNT was approximately 2.8 — dramatically better than thrombolytics. No increase in symptomatic ICH or 90-day mortality.[4]
DEFUSE-3 (2018): Thrombectomy at 6–16 hours using perfusion imaging mismatch criteria. Also strongly positive with NNT of approximately 3.6 for functional independence.[5]
ED implications: Every patient with suspected stroke needs CTA head and neck to evaluate for LVO, even if outside the thrombolytic window. A patient at 12 hours with a large deficit and small core infarct may be a thrombectomy candidate. Contact neurointerventional early. The thrombectomy window is institution-dependent — know your hospital’s protocol and transfer agreements.
Thrombectomy does NOT replace thrombolytics — eligible patients should receive both. Give thrombolytics and proceed to thrombectomy without waiting to see if the thrombolytic works (“drip and ship” or “drip and drive”).
BP Management in Acute Stroke
Pre-thrombolytic: BP must be <185/110 before administering thrombolytics. If above this threshold, treat and reassess — do not delay thrombolysis if BP can be brought into range quickly.[8]
Post-thrombolytic: Maintain BP <180/105 for 24 hours after administration.
No thrombolytics given: Permissive hypertension up to 220/120. Do not aggressively lower BP in acute ischemic stroke without thrombolysis — the hypertension is maintaining perfusion to the ischemic penumbra.[8]
| Agent | Dosing | Notes |
| Nicardipine | 5 mg/hr IV, increase by 2.5 mg/hr q15min, max 15 mg/hr | Preferred — titratable, predictable |
| Labetalol | 10–20 mg IV over 1–2 min, repeat q10–20 min, max 300 mg | Alternative — bolus dosing, less titratable |
| Clevidipine | 1–2 mg/hr IV, double q90sec, max 32 mg/hr | Ultra-short acting, rapid titration |
Pearl: Anticoagulation decisions (aspirin, heparin, clopidogrel) beyond thrombolytics are not emergency department decisions — these belong to the admitting stroke team.
Stroke Syndromes by Vascular Distribution
| Territory | Classic Presentation | Key Features |
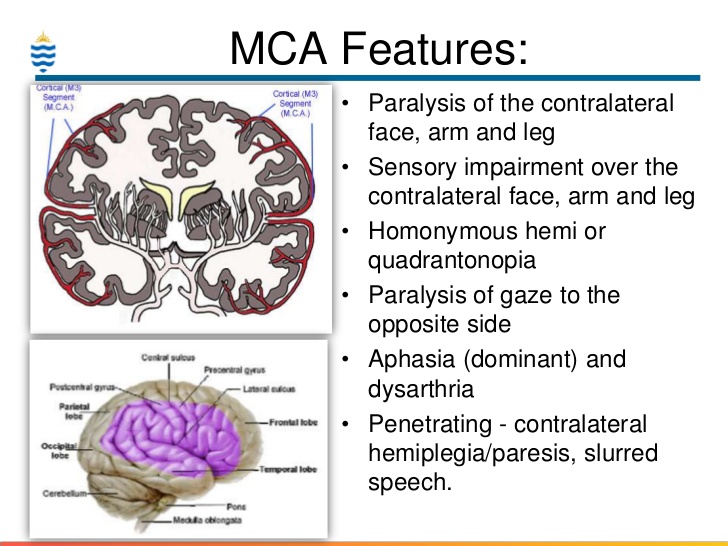
| MCA | Contralateral face + arm > leg weakness and sensory loss | Aphasia (dominant hemisphere), neglect (non-dominant), gaze preference toward lesion. Hyperdense MCA sign on non-contrast CT suggests acute thrombus in the MCA — seen in ~30% of MCA occlusions and may be the earliest CT finding before parenchymal changes are visible. |
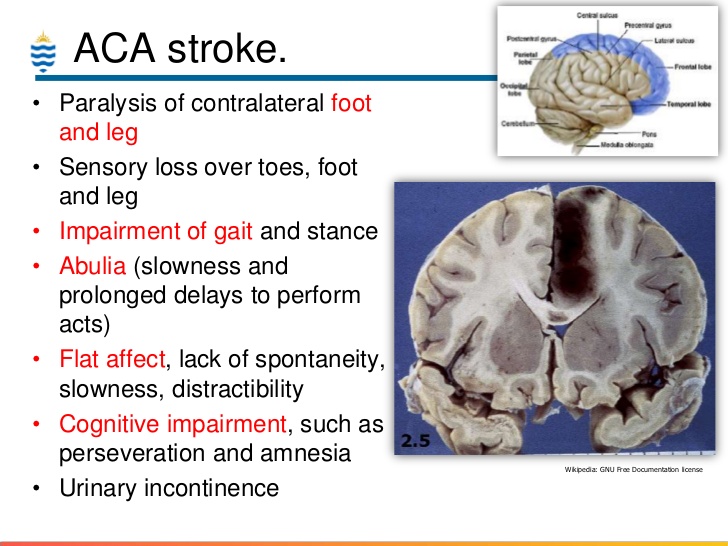
| ACA | Contralateral leg > arm weakness (face/hand spared) | Personality changes, abulia, urinary incontinence |
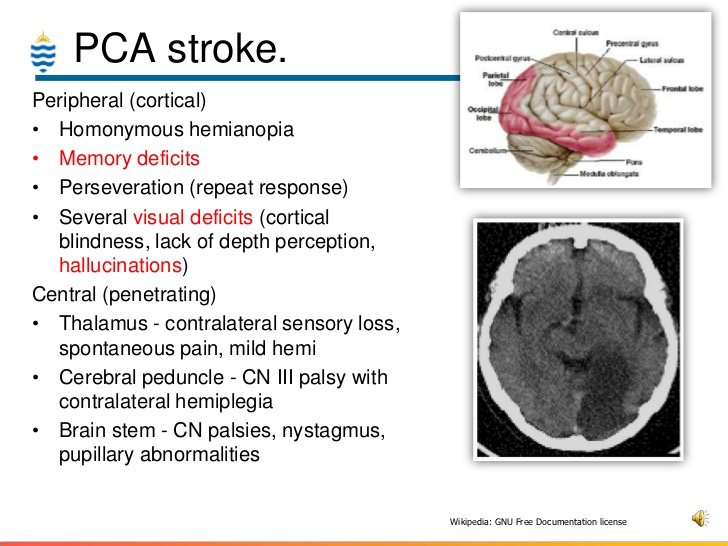
| PCA | Contralateral homonymous hemianopia | Visual field cut without motor deficit, alexia without agraphia (dominant PCA) |
| Lacunar (small vessel) | Pure motor OR pure sensory OR ataxic hemiparesis | No cortical signs (no aphasia, neglect, or visual field cuts). Dysarthria-clumsy hand syndrome. |
| Vertebrobasilar | The 5 D’s: Dizziness, Diplopia, Dysarthria, Dysphagia, Dystaxia | Multiple simultaneous complaints; NOT isolated symptoms. Crossed findings (ipsilateral face + contralateral body) = brainstem localization. |
| PICA (lateral medullary / Wallenberg) | Vertigo, ipsilateral facial pain/numbness, contralateral body sensory loss, ataxia, dysphagia | Ipsilateral Horner syndrome (miosis, ptosis). No motor weakness typically. |
| Basilar artery | Bilateral motor deficits, altered consciousness, “locked-in” syndrome | Quadriplegia with preserved vertical eye movements and blinking. Emergent thrombectomy consideration. |
Peripheral & Atypical Stroke Presentations
Not all strokes present with obvious hemiplegia. Some of the most frequently missed strokes involve isolated or “peripheral-seeming” symptoms. The table below maps these presentations to their vascular territories.
| Presentation | Think About | Vascular Territory |
| Isolated facial droop | Pontine stroke (CN VII nucleus) — upper AND lower face involved (unlike UMN Bell’s pattern) | Basilar perforators |
| Pure sensory loss (numbness only) | Thalamic lacunar infarct — can mimic peripheral neuropathy | PCA / thalamoperforating arteries |
| Isolated vertigo | PICA/AICA cerebellar infarct — HINTS exam is key (see Radiopaedia) | Posterior circulation |
| Acute monocular vision loss | Central retinal artery occlusion — embolic source (carotid), stroke equivalent | Ophthalmic artery (ICA branch) |
| Isolated dysarthria | Lacunar infarct in pons or internal capsule | Small vessel / pontine perforators |
| Leg-predominant weakness (arm/face spared) | ACA territory — frequently missed because “face and arm are fine” | Anterior cerebral artery |
| Bilateral motor deficits | Basilar artery occlusion — do NOT dismiss as “doesn’t lateralize” | Basilar artery |
| Crossed findings (ipsilateral face + contralateral body) | Brainstem stroke — the “crossed” pattern localizes to brainstem, not cortex | Posterior circulation |
| Acute confusion / behavioral change without focal deficit | Non-dominant MCA stroke (right hemisphere) — neglect can present as “confusion” | MCA (non-dominant) |
Pearl: The NIHSS is biased toward anterior circulation and left-hemisphere strokes. A patient with a low NIHSS can still have a significant posterior circulation or right MCA stroke. Clinical suspicion should not rely solely on the NIHSS score.
Wake-Up Stroke & Unknown LKWT
Patients who wake up with deficits or have unknown last known well time are NOT automatically excluded from thrombolysis.
WAKE-UP trial (2018): Patients with unknown onset who had DWI-FLAIR mismatch on MRI (DWI positive but FLAIR negative, suggesting the infarct is likely <4.5 hours old) benefited from IV alteplase with an 11% absolute improvement in favorable outcome at 90 days.[6]
DWI-FLAIR mismatch explained: DWI (diffusion-weighted imaging) shows ischemia within minutes. FLAIR signal change takes roughly 4–6 hours to appear. If DWI is positive but FLAIR is negative, the stroke is likely early enough for thrombolysis.
For thrombectomy: DAWN and DEFUSE-3 criteria use perfusion imaging (CT perfusion or MR perfusion) to identify clinical-imaging mismatch regardless of onset time — extending the window up to 24 hours.[4][5]
ED takeaway: If your hospital has MRI capability, wake-up strokes and unknown LKWT patients should get MRI with DWI/FLAIR (for thrombolytic consideration) and CTA (for LVO/thrombectomy consideration). If no MRI, CT perfusion can provide similar mismatch data for thrombectomy evaluation. Do not dismiss these patients — call neurology early.
Stroke Mimics
Up to 25–30% of initial stroke alerts are ultimately stroke mimics. The most common mimics include:
| Mimic | Distinguishing Features |
| Complex migraine | Gradual symptom onset (“march” over minutes), positive phenomena (scintillating scotoma, tingling), headache, prior history, younger patient |
| Seizure / Todd’s paralysis | Witnessed seizure activity, post-ictal confusion, rapid improvement, known seizure disorder |
| Hypoglycemia | POC glucose is the first test in any stroke alert — resolves with glucose correction |
| Bell’s palsy | Isolated peripheral CN VII (upper AND lower face), no other deficits — but see atypical presentations above for pontine stroke |
| Functional neurologic disorder | Inconsistent exam, positive Hoover sign, give-way weakness — but this is a diagnosis of exclusion after imaging |
| Toxic-metabolic encephalopathy | Diffuse rather than focal findings, identifiable metabolic derangement (Na, hepatic encephalopathy, uremia) |
Pearl: When in doubt, treat it as a stroke. The risk of giving thrombolytics to a stroke mimic is low (symptomatic ICH rate in mimics is <1%). The risk of withholding thrombolytics from an actual stroke is high.
Recrudescence
Recrudescence is the transient worsening or re-emergence of prior stroke deficits triggered by a physiologic stressor — not a new ischemic event. Common triggers include infection (UTI, pneumonia), fever, sedating medications, dehydration, and metabolic derangements.
Cerebral ischemia is considered unlikely when symptom duration >1 hour without a new DWI lesion, there is no suspicion for low-flow TIA from cerebral artery stenosis, AND a recent physiologic stressor is identified.
Differential: TIA (new ischemia), complex migraine, Todd’s paralysis post-seizure, Uhthoff phenomenon (temporary worsening of MS symptoms from increased body temperature).
ED approach: Treat the underlying stressor. If any concern for new ischemia — particularly if deficits are new or different from the prior stroke territory — pursue stroke workup including imaging.
Scoring Tools: NIHSS & RACE
NIH Stroke Scale (NIHSS) — the standard bedside stroke severity assessment. Scores range from 0 to 42. Key thresholds: NIHSS ≥6 suggests LVO until proven otherwise. NIHSS >25 is an exclusion criterion for thrombolysis in the 3–4.5 hour window.[8]
RACE Scale (Rapid Arterial oCclusion Evaluation) — a prehospital/rapid LVO screening tool. Scores range from 0 to 9 (facial palsy, arm motor, leg motor, gaze deviation, aphasia/agnosia). A score ≥5 has a sensitivity of ~85% and specificity of ~68% for LVO. Useful for triage decisions and routing to thrombectomy-capable centers.
Pearl: The NIHSS under-detects posterior circulation strokes and right-hemisphere neglect. A patient with a “low” NIHSS of 3–4 who has basilar symptoms or neglect may still have a devastating stroke. Use clinical judgment alongside the score.
References
- NINDS rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581-1587. PubMed
- Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke (ECASS III). N Engl J Med. 2008;359(13):1317-1329. PubMed
- IST-3 Collaborative Group. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (IST-3): a randomised controlled trial. Lancet. 2012;379(9834):2352-2363. PubMed
- Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct (DAWN). N Engl J Med. 2018;378(1):11-21. PubMed
- Albers GW, Marks MP, Kemp S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging (DEFUSE 3). N Engl J Med. 2018;378(8):708-718. PubMed
- Thomalla G, Simonsen CZ, Boutitie F, et al. MRI-guided thrombolysis for stroke with unknown time of onset (WAKE-UP). N Engl J Med. 2018;379(7):611-622. PubMed
- Menon BK, Buck BH, Singh N, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, non-inferiority trial. Lancet. 2024;404(10449):283-292. PubMed
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines. Stroke. 2019;50(12):e344-e418. PubMed
- Hoffman JR. Thrombolytics for acute ischemic stroke — a critical appraisal. EMRAP (educational resource). EMRAP
- Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384(9958):1929-1935. PubMed
- American Heart Association/American Stroke Association. 2024 Guideline update: tenecteplase for acute ischemic stroke. Stroke. 2024. AHA Journals
