Last reviewed: March 2026
Contents
MDM Templates
Croup — Mild
Child presents with several days of URI symptoms followed by barking cough and low-grade fever. Stridor present only when agitated with mild subcostal retractions. No stridor at rest. Well appearing, no drooling, no muffled voice, no toxic appearance.
History and exam consistent with viral croup (laryngotracheobronchitis). Not consistent with epiglottitis, bacterial tracheitis, peritonsillar abscess, retropharyngeal abscess, foreign body aspiration, or anaphylaxis.[1]
Plan: Dexamethasone 0.6 mg/kg PO (single dose). Observed in ED with improvement. No stridor at rest after treatment.
Disposition: Discharge home. Cool mist humidifier for comfort. Return for stridor at rest, increased work of breathing, inability to tolerate fluids, or worsening symptoms. PCP follow-up in 24-48 hours.
Croup — Moderate to Severe
Child presents with barking cough and inspiratory stridor at rest with significant retractions. Decreased air entry on exam. Appears uncomfortable but maintaining adequate oxygenation.
Presentation consistent with moderate to severe croup. Not consistent with epiglottitis, bacterial tracheitis, foreign body aspiration, or retropharyngeal abscess.[1]
Plan: Dexamethasone 0.6 mg/kg PO/IM. Racemic epinephrine 2.25% (0.05 mL/kg, max 0.5 mL) via nebulizer. Observed for minimum 2-3 hours post-racemic epinephrine for rebound.
If incomplete response: Repeat racemic epinephrine. If requiring ≥2 doses, admission warranted for continued monitoring and potential repeat dosing.[2]
Disposition: If stridor resolved at rest after observation period and no return of symptoms, discharge with close follow-up and strict return precautions. Admit if persistent stridor at rest or requiring repeat racemic epinephrine.
Croup — Impending Respiratory Failure
Child presents with severe stridor, marked retractions, and decreasing air entry. Appearing fatigued with diminishing respiratory effort. Cyanosis or altered mental status may be present.
Presentation consistent with severe croup with impending respiratory failure. Bacterial tracheitis, foreign body, and epiglottitis remain on the differential given severity.[1]
Plan: Racemic epinephrine, dexamethasone 0.6 mg/kg IM, heliox if available (70:30 mix). Prepared for airway management — use endotracheal tube 0.5-1.0 size smaller than age-predicted due to subglottic edema. Pediatric anesthesia and ENT notified for difficult airway backup.
Disposition: Admit to PICU for continuous monitoring and airway management.
Clinical Education
Diagnosis and Ddx
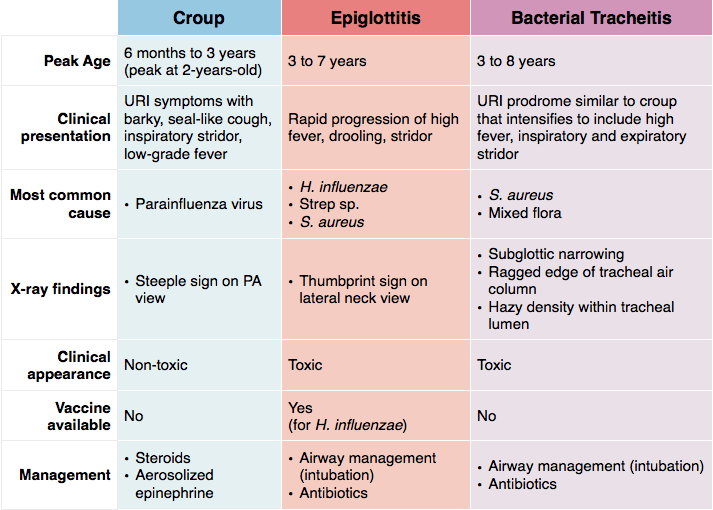
Croup is a clinical diagnosis. Peak incidence age 6 months to 3 years (peak in 2nd year of life), fall and winter predominance. Most commonly caused by parainfluenza virus. Classic triad: barking cough, hoarse voice, inspiratory stridor.[1]
CXR is not needed for typical croup. The “steeple sign” (subglottic narrowing on AP film) is neither sensitive nor specific. Only image if the diagnosis is uncertain or you suspect an alternative.
Avoid agitating the child. Crying worsens dynamic airway obstruction. Examine from across the room first. Let the child stay on the parent’s lap.
Westley Croup Score
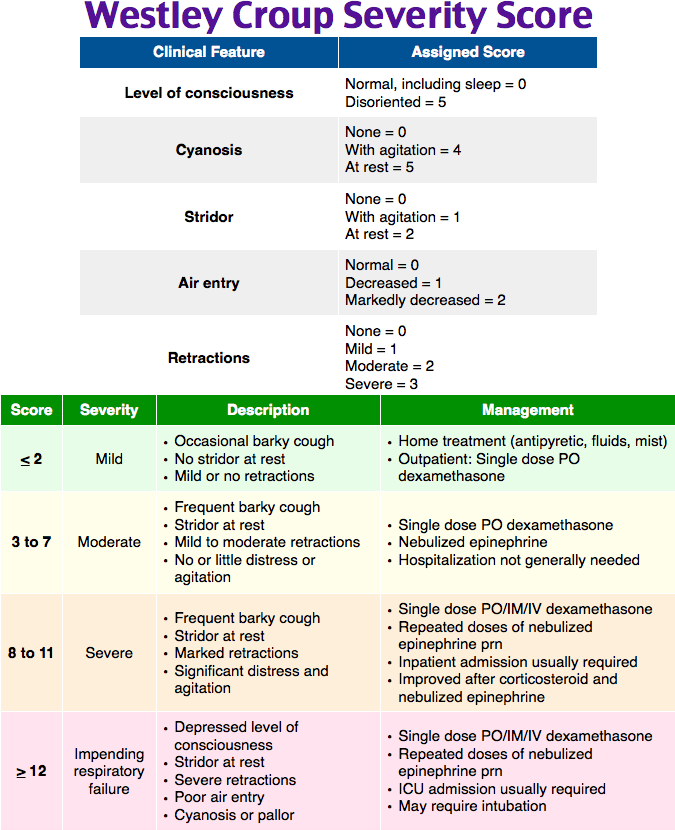
The Westley score stratifies croup severity from 0-17. Useful for standardizing communication and tracking response to treatment.[1]
| Finding | Points |
| Stridor: none (0), with agitation (1), at rest (2) | 0-2 |
| Retractions: none (0), mild (1), moderate (2), severe (3) | 0-3 |
| Air entry: normal (0), decreased (1), markedly decreased (2) | 0-2 |
| Cyanosis: none (0), with agitation (4), at rest (5) | 0-5 |
| Level of consciousness: normal (0), altered (5) | 0-5 |
Mild ≤2, Moderate 3-7, Severe ≥8. Scores ≥8 with cyanosis or altered mental status warrant immediate intervention and PICU preparation.
Dexamethasone
Dexamethasone 0.6 mg/kg PO (single dose, max 16 mg) is first-line for ALL croup — mild, moderate, and severe. Onset at ~6 hours, duration ~72 hours. Shown to reduce ED revisits, need for racemic epinephrine, and hospital admissions.[2]
Oral is preferred over IM (less painful, same efficacy). Give IM only if the child is vomiting or in severe distress. Can mix with flavored syrup to improve palatability.
Lower doses (0.15 mg/kg) may be adequate for mild croup, but 0.6 mg/kg is the most studied dose and is the standard recommendation.[3]
Racemic Epinephrine
Racemic epinephrine is for moderate-to-severe croup with stridor at rest. Onset within 10-30 minutes, duration approximately 2 hours. Works by mucosal vasoconstriction reducing subglottic edema.[2]
Dose: Racemic epinephrine 2.25% — 0.05 mL/kg (max 0.5 mL) nebulized. Alternative: L-epinephrine 1:1000 — 0.5 mL/kg (max 5 mL) nebulized.
Observe 2-3 hours after administration to ensure no rebound worsening. If stridor recurs during the observation period, repeat dosing and plan for admission.
Avoid albuterol — it may worsen edema through vasodilation. Heliox has no strong evidence but may buy time in severe cases as a bridge.
When It’s Not Croup
Epiglottitis: High fever, toxic appearance, muffled (hot potato) voice, drooling, tripoding. Rare post-Hib vaccine but still occurs (H. influenzae type B, Strep, Staph). Do NOT examine the oropharynx — go directly to OR for controlled airway.
Bacterial tracheitis: Looks like croup but fails standard treatment. High fever, toxic appearance, and purulent secretions. Often a secondary bacterial infection after viral croup. Needs IV antibiotics (vancomycin + ceftriaxone) and possible bronchoscopy.
Foreign body: Sudden onset without prodrome in the right age group (6 months to 3 years). Unilateral wheezing or stridor. No fever. CXR with inspiratory/expiratory films or decubitus views.
Retropharyngeal abscess: Neck stiffness, refusal to extend neck, drooling. CT neck with IV contrast for diagnosis.
Disposition Decision Guide
Discharge: Mild croup after dexamethasone. Moderate croup that resolves with racemic epinephrine + dexamethasone and remains clear through 2-3 hour observation. Return precautions for stridor at rest, difficulty breathing, inability to drink, or drooling.
Admit to pediatrics: Requiring ≥2 doses of racemic epinephrine. Persistent stridor at rest despite treatment. Young infant (<6 months) with moderate symptoms. Unreliable follow-up or social concerns.
Admit to PICU: Severe croup with impending respiratory failure. Altered mental status. Requiring continuous racemic epinephrine or heliox. Any child who needed intubation.
