Last reviewed: March 2026
Contents
MDM Templates
Jaundice — Physiologic / Breast Milk
Neonate presents with visible jaundice. Well appearing, feeding well, adequate wet diapers and stooling. No lethargy, poor feeding, or temperature instability. Total bilirubin plots in the low-risk zone on the AAP phototherapy nomogram for age in hours. Direct bilirubin normal (<1 mg/dL).
Presentation consistent with physiologic jaundice or breast milk jaundice. No evidence of hemolytic disease — Coombs negative, hemoglobin and reticulocyte count normal, no hepatosplenomegaly. Not consistent with sepsis, biliary atresia, metabolic disease, or pathologic hemolysis.[1]
Plan: Optimize feeding (lactation support if breastfeeding). Discharge with repeat bilirubin in 24 hours. PCP follow-up for weight check and bilirubin trending. Return for poor feeding, lethargy, or worsening jaundice.
Jaundice — Phototherapy Indicated
Neonate presents with jaundice and total serum bilirubin at or above the phototherapy threshold on the AAP age-specific nomogram. Direct bilirubin normal, confirming unconjugated predominance.
Bilirubin level warrants phototherapy per AAP guidelines. Hemolysis workup obtained — Coombs, CBC with reticulocyte count, blood type. Differential includes ABO incompatibility, G6PD deficiency, hereditary spherocytosis, and inadequate enteral intake with delayed meconium passage. Not consistent with conjugated hyperbilirubinemia, sepsis, or metabolic disease.[1]
Plan: Phototherapy initiated. Bilirubin rechecked every 4-6 hours until trending down and away from treatment threshold. Feeding continued and optimized throughout. Monitor for signs of acute bilirubin encephalopathy (lethargy, hypotonia, high-pitched cry). Admit for phototherapy and monitoring.
If bilirubin approaching exchange transfusion threshold or rising rapidly (>0.5 mg/dL/hour): Intensive phototherapy with preparation for possible exchange transfusion. Neonatology consulted.
Jaundice — Conjugated Hyperbilirubinemia
Neonate presents with jaundice and direct (conjugated) bilirubin >1 mg/dL or >20% of total bilirubin. This is always pathologic in a neonate and requires urgent evaluation.[2]
Conjugated hyperbilirubinemia raises immediate concern for biliary atresia, the leading indication for liver transplantation in children. Differential also includes cholestasis from sepsis, TORCH infections, metabolic disease (alpha-1 antitrypsin deficiency, galactosemia), and neonatal hepatitis. Acholic (pale/clay-colored) stools and dark urine are key clinical clues to biliary obstruction.
Plan: Abdominal ultrasound (triangular cord sign, gallbladder visualization). LFTs, GGT, coagulation studies. Urgent referral to pediatric hepatology and surgery — the Kasai procedure must be performed within 60 days of life for best outcomes. Admit for expedited workup.
Clinical Education
Conjugated vs Unconjugated
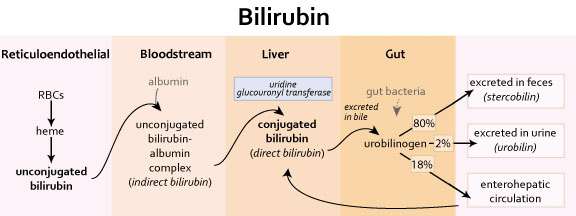
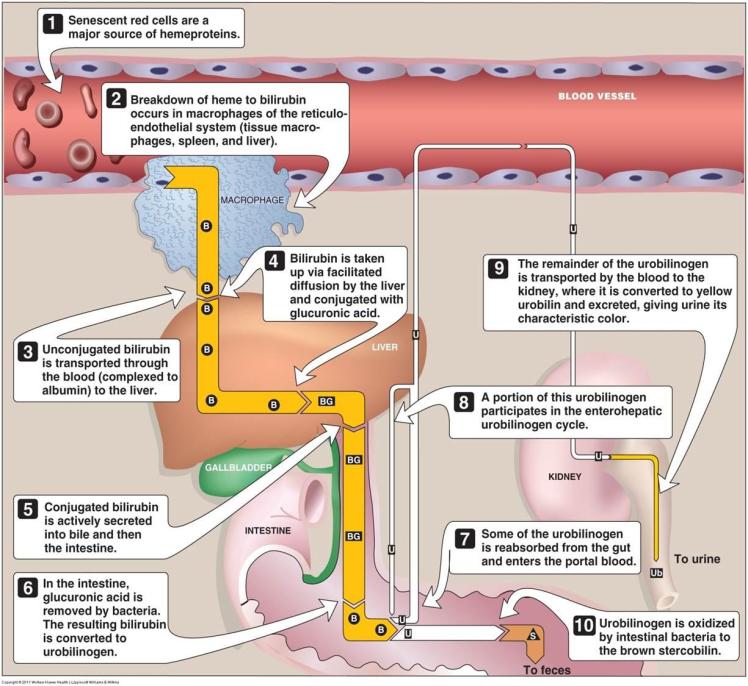
This is the single most important distinction in neonatal jaundice. Unconjugated (indirect) hyperbilirubinemia is common and usually benign — results from immature hepatic conjugation and increased bilirubin load from fetal RBC turnover. Conjugated (direct) hyperbilirubinemia is ALWAYS pathologic and indicates hepatic cholestasis or biliary obstruction.[2]
Rule: direct bilirubin >1 mg/dL or >20% of total = conjugated hyperbilirubinemia. Stop thinking about phototherapy and start thinking about biliary atresia, sepsis, TORCH, and metabolic disease. These are completely different workups and urgencies.
The Bilirubin Nomogram
The AAP phototherapy nomogram determines when to treat. Plot total serum bilirubin against postnatal age in hours. Risk zones are stratified by gestational age and presence of neurotoxicity risk factors (isoimmune hemolytic disease, G6PD deficiency, asphyxia, sepsis, acidosis, albumin ❤ g/dL).[1]
The nomogram is NOT used for: conjugated hyperbilirubinemia (any elevation warrants investigation), bilirubin obtained before 24 hours of age (jaundice <24 hours old is always pathologic and suggests hemolysis), or premature infants <35 weeks (separate thresholds apply).
Hemolytic Causes
ABO incompatibility is the most common hemolytic cause of neonatal jaundice (mother type O, baby type A or B). Usually mild, but can cause rapid bilirubin rise requiring aggressive phototherapy. Positive direct Coombs, elevated reticulocyte count, declining hemoglobin. IVIG may reduce need for exchange transfusion.[1]
G6PD deficiency is an important nonimmune hemolytic cause, particularly in African, Mediterranean, and Asian infants. Can cause sudden severe hyperbilirubinemia, often triggered by infection or oxidative stress. Coombs negative. Screen with quantitative G6PD enzyme level.
Rh incompatibility is now rare due to RhoGAM prophylaxis but when present causes severe hemolysis. Hereditary spherocytosis presents with jaundice, anemia, and spherocytes on smear.
Biliary Atresia
Biliary atresia is the can’t-miss diagnosis in neonatal jaundice. Progressive obliteration of extrahepatic bile ducts leading to cirrhosis and liver failure if untreated. Leading indication for pediatric liver transplantation. The Kasai hepatoportoenterostomy within 30-60 days of life offers the best chance of preserving native liver function.[3]
Clinical clues: conjugated hyperbilirubinemia, acholic (pale/clay-colored) stools, dark urine, hepatomegaly. The infant may initially appear well, making early detection challenging. Abdominal ultrasound looks for the triangular cord sign at the hepatic hilum and absent or abnormal gallbladder.
Any neonate with conjugated hyperbilirubinemia and acholic stools needs same-day referral to pediatric hepatology and surgery. Every day of delay worsens outcomes.
Kernicterus
Kernicterus is bilirubin encephalopathy from severe unconjugated hyperbilirubinemia. Unconjugated bilirubin crosses the blood-brain barrier and deposits in basal ganglia, brainstem, and cerebellum. Risk increased by prematurity, sepsis, acidosis, hypoalbuminemia, and hemolysis.[1]
Acute bilirubin encephalopathy presents with: lethargy, poor feeding, hypotonia, high-pitched cry, opisthotonus, and seizures. This is reversible with emergent phototherapy and exchange transfusion. Chronic kernicterus (permanent) causes choreoathetoid cerebral palsy, sensorineural hearing loss, gaze palsy, and intellectual disability.
Prevention is the strategy: universal bilirubin screening before discharge, risk stratification with the nomogram, and close outpatient follow-up with repeat bilirubin measurement.
Disposition
Admit: Bilirubin at or above phototherapy threshold. Evidence of hemolytic disease with rapidly rising bilirubin. Any conjugated hyperbilirubinemia requiring expedited workup. Signs of acute bilirubin encephalopathy. Inadequate follow-up arrangements.
Discharge: Bilirubin in low-risk zone with reliable 24-hour follow-up for repeat level. Feeding well with adequate output. No hemolysis on labs. Clear return precautions for poor feeding, lethargy, or worsening jaundice.
References
- American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004;114(1):297-316. PubMed
- Moyer V, Freese DK, Whitington PF, et al. Guideline for the evaluation of cholestatic jaundice in infants. J Pediatr Gastroenterol Nutr. 2004;39(2):115-128. PubMed
- Hartley JL, Davenport M, Kelly DA. Biliary atresia. Lancet. 2009;374(9702):1704-1713. PubMed
