Last reviewed: March 2026
Contents
MDM Templates
Hemarthrosis
Patient with known hemophilia presents with acute joint pain, swelling, and decreased range of motion consistent with hemarthrosis. They deny head trauma, GI bleeding, hematuria, or other sites of hemorrhage. They are hemodynamically stable.
Presentation is consistent with acute hemarthrosis, the most common manifestation of hemophilia bleeding. History and exam lower suspicion for septic arthritis, fracture, or compartment syndrome. Joint infection remains in the differential and should be reconsidered if fever develops or symptoms fail to improve with factor replacement.
Plan: Factor replacement administered in ED per hematology guidance. Ice, elevation, immobilization of affected joint. Pain managed with acetaminophen and opioids as needed — NSAIDs avoided due to platelet dysfunction risk.
Disposition: Discharge with hematology follow-up within 24 hours if symptoms improving after factor infusion. Return precautions for worsening swelling, fever, or new bleeding sites.
Admit if: Inadequate response to factor replacement, concern for inhibitor, recurrent hemarthrosis with joint destruction, or inability to obtain outpatient factor infusions.
Major / Life-Threatening Bleed
Patient with known hemophilia presents with concern for significant hemorrhage involving ***. Given the bleeding diathesis, even seemingly minor mechanisms can produce life-threatening hemorrhage. Head trauma in hemophilia patients warrants factor replacement before imaging.
Presentation warrants emergent factor replacement to 100% activity level prior to further workup. History and exam raise concern for hemorrhage requiring immediate correction of coagulopathy.
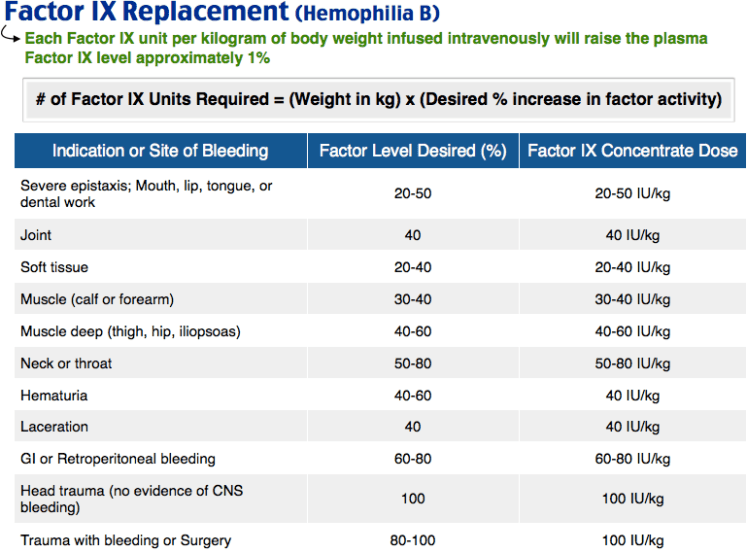
Plan: Factor replacement to 100% activity — Hemophilia A: Factor VIII 50 IU/kg IV. Hemophilia B: Factor IX 100 IU/kg IV. Hematology consulted emergently.
Disposition: Admit. ICU if intracranial hemorrhage, retroperitoneal bleed, or hemodynamic instability.
Clinical Education
Factor Replacement Dosing
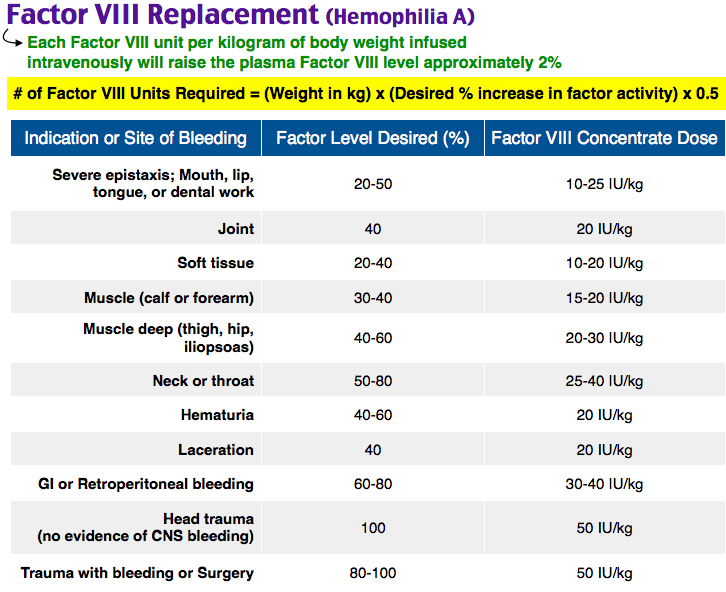
The key formula for Factor VIII: 1 IU/kg raises circulating factor level by 2%. Target activity levels depend on bleed severity:[1]
| Bleed Type | Target Activity | Factor VIII Dose |
| Minor (hemarthrosis, superficial) | 30-50% | 15-25 IU/kg |
| Major (GI, retroperitoneal, deep muscle) | 50-80% | 25-40 IU/kg |
| Life-threatening (ICH, airway, surgery) | 80-100% | 50 IU/kg |
Factor IX dosing is different: 1 IU/kg raises activity by only ~1% (half the potency of Factor VIII). For life-threatening bleeds, give Factor IX 100 IU/kg to achieve 100% activity.[1]
Give factor FIRST, image SECOND. In head trauma, do not wait for CT results to administer factor replacement. The factor should be infusing while the patient is in the scanner.
Hemophilia A vs B
Hemophilia A (Factor VIII deficiency) accounts for ~80% of cases. Hemophilia B (Factor IX deficiency, “Christmas disease”) accounts for ~20%. Both are X-linked recessive. Clinically indistinguishable — the distinction matters only for which factor to replace.[2]
Lab findings: Elevated PTT with normal PT and normal platelet count. The PTT corrects on mixing study (distinguishing from an inhibitor). Factor activity levels classify severity: severe (<1%), moderate (1-5%), mild (5-40%).[2]
Cryoprecipitate contains Factor VIII, fibrinogen, vWF, and Factor XIII — it is NOT helpful for Factor IX deficiency (Hemophilia B). For Hemophilia B, use recombinant Factor IX or PCC (prothrombin complex concentrate, which contains Factors II, VII, IX, and X).[1]
Patients with Inhibitors
Inhibitors are antibodies against replacement factor that develop in ~30% of severe Hemophilia A patients and ~5% of Hemophilia B patients. Standard factor replacement is ineffective in these patients.[3]
Bypass therapy options: Activated prothrombin complex concentrate (FEIBA 50-100 IU/kg) or recombinant Factor VIIa (NovoSeven 90 mcg/kg). Hematology consultation is essential — these patients require specialized management.
Emicizumab (Hemlibra): A bispecific antibody that mimics Factor VIII function, now widely used for prophylaxis in Hemophilia A patients with inhibitors. Patients on emicizumab may still need bypass agents for breakthrough bleeds, but their baseline bleeding risk is dramatically reduced.[3]
Adjunctive Therapies
DDAVP (desmopressin) 0.3 mcg/kg IV: Releases endogenous Factor VIII and vWF stores. Useful for mild Hemophilia A (baseline factor >5%) and minor bleeds. Not effective in Hemophilia B. Tachyphylaxis occurs after 2-3 doses.[1]
Tranexamic acid (TXA) 1g IV or 1.3g PO TID: Useful adjunct for mucosal bleeding (oral, nasal, menstrual). Avoid in hematuria (risk of ureteral clot obstruction).[1]
Pain management: Acetaminophen and opioids. Avoid NSAIDs (impair platelet function). Avoid IM injections (hematoma risk).
References
- Srivastava A et al. WFH Guidelines for the Management of Hemophilia, 3rd Edition. Haemophilia. 2020;26(Suppl 6):1-158. PubMed
- Mannucci PM, Tuddenham EG. The Hemophilias — From Royal Genes to Gene Therapy. N Engl J Med. 2001;344(23):1773-1779. PubMed
- Oldenburg J et al. Emicizumab Prophylaxis in Hemophilia A with Inhibitors (HAVEN 1). N Engl J Med. 2017;377(9):809-818. PubMed
