Hypoglycemia: Management Decision Models
Emergency Medicine Clinical Education
Last reviewed: March 2026
Contents
Clinical Templates
Hypoglycemia — Insulin User
This is the most common presentation of hypoglycemia in the ED. The typical scenario involves a patient on insulin—either subcutaneous or pump-based—who has taken their usual dose but then skipped a meal, vomited after taking their injection, or had unexpected exertion. The pathophysiology is straightforward: insulin delivery continues without adequate carbohydrate intake, driving glucose into cells and hepatic glucose production downward.
On arrival the patient is often symptomatic with autonomic signs: tremor, diaphoresis, tachycardia, anxiety. Neuroglycopenic symptoms—confusion, combativeness, altered mental status—correlate with severity and duration. Capillary glucose is typically 40–70 mg/dL at presentation.
My approach: After drawing glucose, I immediately give IV dextrose (see Dextrose Formulations). If IV access is delayed or impossible, I give glucagon IM. Once glucose is restored and the patient is able to take PO, I encourage a simple snack—juice, crackers, fast-acting carbs—to prevent rebound hypoglycemia as the dextrose bolus wears off.
I explain the incident to the patient and check in with their home insulin regimen. Did they miss a meal? Take extra insulin? Most insulin users are well aware of their condition; many self-correct before arriving. The episode often reflects medication misadventure rather than new pathology.
If hypoglycemia is severe, prolonged, or recurrent despite treatment: I admit for closer observation and adjustment of insulin dosing, especially in the setting of renal failure, new infection, or medication changes that may alter insulin requirement.
Typical disposition: Home after symptom resolution, capillary glucose >100 mg/dL on reassessment, ability to maintain oral intake, and reliable follow-up with primary care or endocrinology.
Hypoglycemia — Sulfonylurea / Oral Antihyperglycemic User
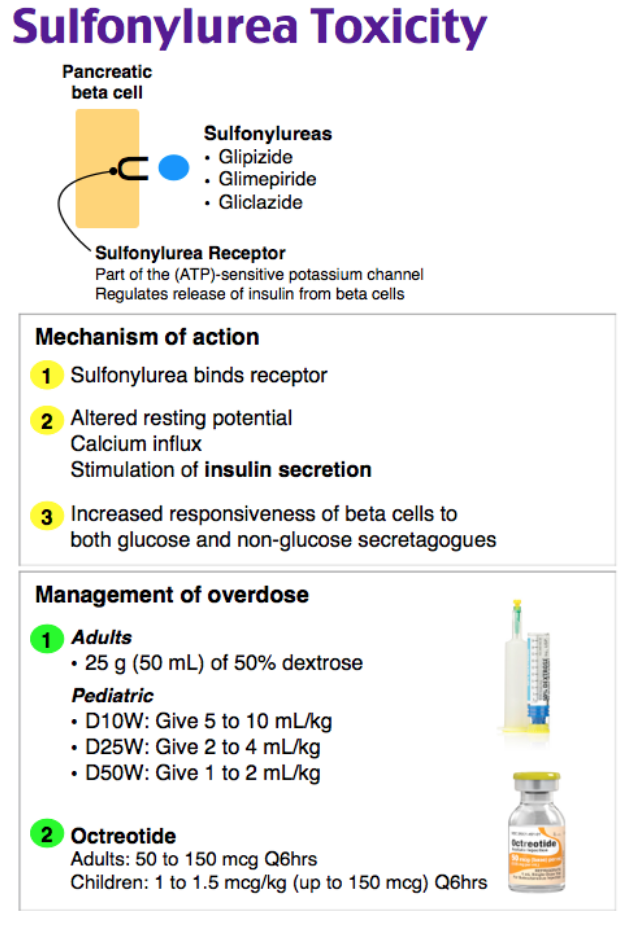
Sulfonylureas (glyburide, glipizide, glimepiride) and meglitinides (repaglinide, nateglinide) cause hypoglycemia through sustained insulin secretion independent of glucose feedback. This is a fundamentally different mechanism from insulin: the drug forces the pancreas to pour out insulin regardless of blood glucose, making these episodes more severe and more prolonged than insulin-induced hypoglycemia. Recurrence is common—the drug is still on board.
Glyburide is the worst offender, with the longest duration of action and highest rate of severe hypoglycemic episodes. Glipizide is somewhat safer due to shorter half-life and more glucose-dependent secretion, but all sulfonylureas carry risk.
Initial treatment is identical to insulin hypoglycemia—IV dextrose immediately. However, disposition is entirely different. All sulfonylurea hypoglycemia requires admission. These patients must be observed for recurrence, have frequent reassessment of glucose, and receive IV dextrose infusion if hypoglycemia recurs despite PO intake. I do not send these patients home after a single dextrose bolus.
I strongly consider octreotide (see Sulfonylurea Pearls) for sustained hypoglycemia, recurrence, or when IV dextrose requirement is high. This agent rapidly suppresses insulin secretion and can prevent the exhausting cycle of repeated hypoglycemic episodes and repeated dextrose boluses overnight.
On the ward or ICU, the patient receives D5W or D10W infusion to maintain glucose >100 mg/dL, frequent glucose checks (every 30–60 min initially), and octreotide if indicated. The home sulfonylurea is discontinued. Once stable for several hours on infusion alone with glucose >150 mg/dL, a trial of PO carbs may be attempted.
If the patient is elderly, frail, or has comorbid renal/hepatic disease: The indication for admission is even stronger, and I am more likely to use octreotide given the high risk of recurrence and harm from repeated lows.
Hypoglycemia — Non-Diabetic Patient
A truly hypoglycemic non-diabetic patient presents a diagnostic puzzle. Whipple’s triad must be documented: (1) symptoms of hypoglycemia, (2) low measured glucose at the time of symptoms, and (3) relief of symptoms after raising glucose. All three elements are essential—patients often report historical lows that were never measured, which does not constitute true hypoglycemia.
The workup is focused on ruling out life-threatening causes: adrenal insufficiency, sepsis, liver failure, acute renal failure. I check cortisol (8 AM if possible, but any time cortisol <10 mcg/dL is concerning), electrolytes with particular attention to sodium (SIADH?), liver function, lactate, beta-hydroxybutyrate, and insulin level with C-peptide at the moment of hypoglycemia if possible. Urine ketones help distinguish between insulin-mediated suppression (beta-OH butyrate low, urine ketones present) versus impaired ketogenesis (hepatic disease, sepsis).
If no obvious cause emerges—no adrenal insufficiency, no shock, no hepatic failure, no renal failure—and the patient is otherwise well appearing, I admit for continuous glucose monitoring, repeat fasting labs, and consideration of an insulin tolerance test or supervised fast to diagnose insulinoma or factitious hypoglycemia (surreptitious insulin or sulfonylurea injection).
Causes to consider: endocrine—adrenal insufficiency, hypothyroidism, growth hormone deficiency; hepatic—cirrhosis, fulminant hepatitis, glycogen storage disease; sepsis—overwhelming infection consuming glucose; renal—uremia, reduced gluconeogenesis; neoplastic—insulinoma; medication—salicylates, alcohol; factitious—self-injected insulin or oral sulfonylurea.
If cortisol is low: I give dexamethasone 4 mg IV after drawing cortisol, do not wait for ACTH, and involve endocrinology urgently for adrenal assessment and long-term steroid replacement.
Dextrose Formulations: D50 vs. D10
For decades, D50W (50% dextrose) was the standard ED bolus for symptomatic hypoglycemia. One 25 mL bolus (12.5 g dextrose) raises capillary glucose 50–100 mg/dL depending on the patient’s weight and volume status. The advantage was speed and volume efficiency—one syringe, one push.
However, evidence increasingly favors D10W (10% dextrose) delivered IV, particularly in resource-rich settings. D10W is physiologically more similar to endogenous glucose supplementation. It causes less hyperglycemia overshoot, reduces the rate of osmotic shift-induced cerebral edema (rare but catastrophic), and—critically—is vastly safer if extravasation occurs. D50 causes severe tissue injury and can require fasciotomy; D10 is benign even in the subcutaneous space.
Titration of D10W is straightforward: infuse 2–5 mL/kg (~150–250 mL for a typical adult) and recheck glucose every 5–10 minutes, stopping when glucose reaches ≥70 mg/dL. The infusion takes 2–3 minutes but eliminates the risk of bolus extravasation and gives better glucose control. Many modern EDs now stock D10W as their preferred formulation.
If D50W is used, push is faster but extravasation risk demands peripheral IV placement in large antecubital veins with good flow. Central lines are safer, but not always immediately available. After any dextrose bolus, I recheck glucose at 5 min and again at 15 min to ensure sustained correction and catch any recurrent decline early.
Glucagon IM is the backup when IV access is absent or delayed. Standard dose is 1 mg IM (given as 1 U/kg for children). Onset is 5–15 minutes. Glucagon works only if the patient has hepatic glycogen stores—it is ineffective in prolonged fasting, liver failure, or after massive dextrose has been given. I always obtain IV access once glucagon is given and follow with dextrose, since glucagon’s effect wears off within 30–60 minutes.
Follow-up infusion: After any dextrose bolus in a critically ill or sulfonylurea-treated patient, I hang a D5W or D10W drip set to 100–150 mL/h to prevent rebound hypoglycemia. This is especially important overnight when frequent reassessment is harder.
Sulfonylurea Hypoglycemia: Octreotide and Admission Criteria
Octreotide is a somatostatin analog that rapidly inhibits pancreatic insulin secretion. In sulfonylurea-induced hypoglycemia, it is the only agent that addresses the root problem: forcing the pancreas to stop dumping insulin. Without it, patients cycle between dextrose boluses and recurrent lows all night.
Dosing: 50 mcg (0.05 mg) subcutaneously every 6 hours. Onset is 10–30 minutes. Some references suggest a 100 mcg initial dose for faster suppression, but 50 mcg q6h is standard in most EDs and endocrinology literature. After the first dose, most patients are stable; subsequent doses prevent recurrence.
Mechanism: Octreotide binds somatostatin receptor 2, which is abundant on pancreatic beta cells. Activation suppresses intracellular calcium signaling required for exocytosis of insulin granules. Unlike glucagon (which only works transiently and requires hepatic stores), octreotide directly turns off the pathologic insulin secretion.
Indications for octreotide:
- Any sulfonylurea hypoglycemia with recurrence of low glucose within 30 minutes of dextrose bolus
- High dextrose requirement (>25 g in first 30 min) indicating severe insulin excess
- Elderly or frail patient where frequent lab draws and IV therapy are high burden
- Overnight admission where close monitoring is impractical
Which sulfonylureas are most dangerous? Glyburide > glipizide > glimepiride > repaglinide in terms of hypoglycemia risk and duration. Glyburide binds more tightly to beta cell sulfonylurea receptors and has a 10–24 hour half-life. Glipizide is shorter-acting (4–7 hours) and slightly more glucose-responsive, but still poses risk. Meglitinides (repaglinide, nateglinide) are rapid-onset, short-duration agents; hypoglycemia from these is less severe and less likely to recur.
Admission criteria for sulfonylurea hypoglycemia: Admit all patients. No exceptions. The risk of recurrence and the severity of unrecognized nocturnal hypoglycemia in an elderly or frail patient are too high. Even young, well patients warrant at least several hours of observation and frequent glucose checks. If the ED is extremely busy and admission is not logistically feasible, arrange for very close same-day follow-up (within 4 hours) with primary care and frequent phone checks, but this is not ideal.
On the ward: Continue D5W or D10W infusion. Recheck glucose every 30–60 minutes. If glucose stays >120 mg/dL for 2 hours and the patient has taken food, discontinue infusion and monitor q2h overnight. Consider octreotide if any recurrent lows occur. Discontinue the home sulfonylurea. Consult endocrinology or primary care for regimen adjustment before discharge.
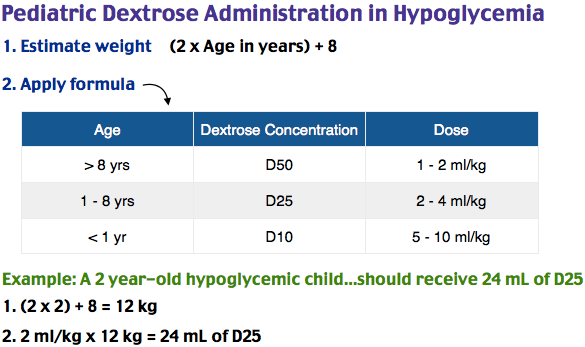
Pediatric Hypoglycemia
Dosing of dextrose by age:
- Neonates and infants (<1 year): 2–5 mL/kg of D10W IV (target 100–150 mL total). Maximum 12.5 g dextrose per bolus.
- Young children (1–8 years): 2 mL/kg of D25W IV or 5 mL/kg of D10W IV. Titrate to glucose ≥70 mg/dL.
- Older children and adolescents (>8 years): Weight-based dosing or standard adolescent/adult approach: 0.5 g/kg dextrose IV (e.g., 25–35 mL of D50W for a 50 kg child).
- Glucagon IM if no IV: 0.03 mg/kg IM (max 1 mg). May repeat in 10–15 minutes if glucose not rising.
Neonatal hypoglycemia (first 48 hours of life): Is common and often benign in healthy term infants. Asymptomatic hypoglycemia (glucose <40 mg/dL without symptoms) may not require IV dextrose if the infant can feed and glucose checks show rising trend. However, if the infant is symptomatic (jitteriness, poor feeding, seizures) or glucose <25 mg/dL, give D10W 2–5 mL/kg IV. The key is always consider sepsis in a neonate with hypoglycemia—hypoglycemia may be the first sign of overwhelming infection. Check CBC with differential, blood culture, lactate, and consider empiric antibiotics after cultures.
Congenital adrenal hyperplasia (CAH) screening: A neonate or young child presenting with unexplained hypoglycemia warrants checking serum sodium and potassium immediately. CAH (21-hydroxylase deficiency being most common) causes hypoglycemia via impaired cortisol synthesis and hypotension via salt wasting. Hyponatremia and hyperkalemia are the red flags. Obtain a cortisol level and ACTH; if cortisol is low (<5 mcg/dL), give dexamethasone 0.5 mg IV (weight-based dosing) and contact endocrinology urgently. Do not wait for confirmatory testing (17-hydroxyprogesterone).
Pediatric non-diabetic hypoglycemia: In children, hypoglycemia is more often due to hepatic dysfunction (cirrhosis, glycogen storage disease, acute viral hepatitis), sepsis, growth hormone deficiency, or adrenal insufficiency than to insulinoma or factitious injection. Obtain urine and serum ketones, insulin level with C-peptide at the moment of low glucose if possible, liver function, and lactate. Fasting hypoglycemia in a child warrants admission for supervised fasting labs and endocrinology workup.
Non-Diabetic Hypoglycemia: Diagnosis and Workup
Any patient presenting with documented hypoglycemia (glucose measured at the time of symptoms) and no history of diabetes or insulin use requires a focused workup. The differential is broad but manageable with a systematic approach.
Whipple’s triad (all three must be present):
- Symptoms of hypoglycemia (autonomic: tremor, diaphoresis, palpitations, anxiety; neuroglycopenic: confusion, seizure, altered mental status)
- Measured blood glucose <55 mg/dL at the time of symptoms
- Relief of symptoms after raising glucose (or empiric IV dextrose if glucose was not rechecked)
If the patient reports “feeling shaky and weird” and checks finger stick at home finding 60 mg/dL, but feels fine now, this does not constitute true hypoglycemia without documented symptoms at the time of low reading.
Laboratory evaluation at the moment of hypoglycemia: Ideally, labs are drawn when glucose is genuinely low. Practically, this is often impossible in the ED. However, at minimum:
- Serum glucose (VG or lab; capillary may be falsely low)
- Insulin and C-peptide — If insulin is detectable and C-peptide is also detectable, the pancreas is secreting (either from ongoing sulfonylurea, endogenous insulinoma, or factitious insulin injection). If insulin is high but C-peptide is low or absent, factitious insulin is likely. If both are suppressed, rule out insulinoma.
- Cortisol (8 AM if possible; any cortisol <10 mcg/dL is abnormal and warrants dexamethasone)
- Electrolytes (Na, K, Cl—low Na/high K suggests CAH or adrenal insufficiency)
- Liver function (AST, ALT, bilirubin, albumin, PT/INR)
- Lactate (elevated in sepsis, shock, severe liver disease)
- Beta-hydroxybutyrate or urine ketones (helps distinguish normal ketogenesis from impaired ketogenesis)
Differential diagnosis:
Adrenal insufficiency: Cortisol <10 mcg/dL in a hypoglycemic patient is adrenal insufficiency until proven otherwise. This is a medical emergency. Give dexamethasone 4 mg IV immediately (do not wait for ACTH), supportive care (IV fluids, ICU monitoring), and contact endocrinology. Causes include primary adrenal failure (autoimmune, infection, hemorrhage), secondary (pituitary or hypothalamic disease), or acute adrenal crisis in known Addison's disease.
Hepatic failure: Marked elevation of transaminases (often >1000), coagulopathy (INR >1.5), elevated bilirubin, and low albumin. Hypoglycemia results from impaired gluconeogenesis and reduced glycogen stores. Manage hypoglycemia with dextrose, admit, and treat underlying liver disease (discontinue hepatotoxins, consider lactulose, monitor for encephalopathy).
Sepsis: Hypoglycemia in the context of fever, elevated lactate, altered mental status, and hemodynamic instability. Glucose is consumed by activated immune cells; hypoglycemia may precede shock. Give dextrose, broad-spectrum antibiotics, and aggressive resuscitation.
Renal failure: Uremia impairs renal gluconeogenesis (normally 90% of endogenous glucose production comes from liver, 10% from kidney, but in renal failure the kidney’s contribution is abolished). Creatinine is markedly elevated. Treat hypoglycemia and dialyze; hypoglycemia often resolves once uremia is corrected.
Insulinoma: Rare neuroendocrine tumor secreting unregulated insulin. Hypoglycemia occurs with fasting or exertion. At the moment of hypoglycemia, insulin is elevated (often >10 microIU/mL) and C-peptide is also elevated (unlike factitious insulin injection). Diagnosis requires supervised fasting test or imaging (CT, MRI, endoscopic ultrasound). Admit for fasting labs and endocrinology workup.
Factitious hypoglycemia: Patient self-injects insulin (or less commonly, takes oral sulfonylureas secretly). At the moment of hypoglycemia, insulin is high but C-peptide is suppressed (because the exogenous insulin shuts down the pancreas). Surreptitious sulfonylurea shows high insulin and high C-peptide with urine metabolites of sulfonylurea detectable. Urine screen and toxicology may help. This is often a psychiatric issue; approach sensitively and involve social work and psychiatry.
Alcohol-induced hypoglycemia: Ethanol inhibits hepatic gluconeogenesis. Hypoglycemia is usually mild and corrects quickly with dextrose, but severe hypoglycemia can occur in malnourished patients or those with liver disease. Thiamine 100 mg IV before or concurrent with dextrose (prevents Wernicke encephalopathy if patient is at risk).
Disposition: Who Goes Home, Who Gets Admitted
Discharge home (after hypoglycemia correction and reassessment):
- Insulin user with clear precipitant (missed meal, excessive exertion) who is now alert, tolerating PO, and capillary glucose ≥100 mg/dL on repeat checks 15 and 30 min after intervention
- Reliable follow-up: Patient has phone number for endocrinologist or primary care, will call within 24 hours, lives with someone who can monitor them or has no safety concerns about living alone
- Education provided: Counseled on the event, given written materials on insulin adjustment, advised on recognition of early warning signs
- No recurrent lows: One episode with clear cause and full recovery. If hypoglycemia recurs despite dextrose, admit.
Admission required:
- All sulfonylurea hypoglycemia — no exceptions (see Sulfonylurea Pearls)
- Recurrent hypoglycemia despite IV dextrose and PO intake (suggest occult sulfonylurea, insulinoma, or impaired insulin clearance)
- Severe or prolonged altered mental status (risk of cerebral edema, aspiration, ICU monitoring needed)
- No clear cause identified — non-diabetic hypoglycemia with unrevealing ED workup warrants admission for continuous glucose monitoring, repeat labs, and supervised fasting test
- Elderly or frail patient with insulin hypoglycemia and no reliable follow-up or social support
- Complicated comorbidities (recent MI, heart failure, renal failure, liver disease) — hypoglycemia is a stress on the system; safer to admit and observe
- Unsafe discharge: Living alone, impaired cognition (dementia, developmental delay, intoxication), unsafe home, unreliable follow-up
Observation unit as alternative: Some EDs have observation units allowing 4–8 hour monitoring with serial glucose checks and PO trial. This may be appropriate for a well-appearing insulin user who is not yet safe to discharge but does not require full inpatient admission. Requires reliable follow-up arrangement before discharge.
Insulin Pump Pearls
What insulin is in the pump? Modern insulin pumps deliver only rapid-acting insulin: lispro (Humalog), aspart (NovoLog), or glulisine (Apidra). These were designed for pump use because of their rapid onset and offset. There is no basal insulin in the pump reservoir in the way there is with insulin pens or syringes (e.g., glargine, detemir, degludec); instead, the pump delivers rapid-acting insulin in very small increments (0.5–2 units per hour) to mimic basal secretion.
Hypoglycemia in a pump user: Treat immediately with IV dextrose, the same as any insulin user. The hypoglycemia is from the pump’s delivery plus missed meals or unexpected exertion. After glucose recovery, I do not automatically recommend disconnecting the pump. The pump is actually safer than syringes for most patients because it delivers insulin continuously in small amounts and has safety features (low glucose suspend, predictive alarms). Disconnecting the pump removes the basal insulin delivery and risks hyperglycemia and DKA if the pump is not restarted promptly.
Exception: Disconnect the pump if the patient is in or at high risk of diabetic ketoacidosis (very high glucose, ketonuria, altered mental status, hemodynamic instability). In DKA, the pump’s rapid-acting insulin is ineffective and dangerous; the patient needs IV insulin in a monitored setting. Once DKA is resolved, restart the pump.
Pump interrogation basics: If available in the ED (and only if you have training), you can wirelessly access or manually review the pump’s screen to see the last bolus given (time, amount), current basal rate, insulin remaining, and glucose history if the pump has CGM capability. This helps confirm that the pump did not malfunction and clarifies the timeline. However, this is secondary to immediate treatment. Do not delay dextrose to interrogate a pump.
Pump malfunction or unexplained recurrent lows: If a patient with a pump has multiple hypoglycemic episodes despite adequate carbohydrate intake, suspect pump malfunction (delivery failure, infusion set clog, battery failure, software glitch). Contact the pump company’s 24-hour support line (Medtronic, Tandem, Insulet, etc.) and consider switching to pen-based insulin temporarily while the pump is serviced.
Admission criteria for pump users: Hypoglycemia in a pump user warrants the same admission criteria as any insulin user (see Disposition). If the pump has malfunctioned, admission is more likely because the patient cannot safely use insulin at home without a working pump or backup pen/syringe supply.
References
- American Diabetes Association. Standards of Medical Care in Diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S1–S298. PubMed
- Cryer PE. Hypoglycaemia: the limiting factor in the glycaemic management of Type I and Type II diabetes. Diabetologia. 2002;45(7):937–948. PubMed
- Grunberger G, Sherwin RS, Simonson DC. Insulin, glucagon, and somatostatin in the regulation of nutrient homeostasis. Endocrinology. 1978;102(4):1193–1199. PubMed
- Kalra S, Kalra B, Agrawal N. Octreotide in hypoglycaemia unawareness: a case series and literature review. J Diabetes Metab Disord. 2013;12(1):48. PubMed
- Kline JA, Gonzales F, Diercks DB. Intravenous dextrose in the hypoglycemic patient: pharmacokinetics and safety considerations. Ann Emerg Med. 2012;59(3):180–187. PubMed
- Iftikhar H, Mahgoub M, Al Ansari A, et al. Octreotide for prevention of recurrent hypoglycemia in patients with sulfonylurea overdose. Crit Care Med. 2016;44(3):e175–e178. PubMed
- Triplitt C, Reasner C, Draznin B. Sulfonylureas: meglitinides, and other agents. In: Therapy for Diabetes Mellitus and Related Disorders. 6th ed. American Diabetes Association; 2017:102–119.
- Cornblath M, Hawdon JM, Williams AF, et al. Controversies regarding definition of neonatal hypoglycemia: suggested operational thresholds for glucose concentrations. Pediatrics. 2000;105(5):1141–1145. PubMed
- Whipple AO. The surgical therapy of hyperinsulinism. J Int Chir. 1938;3:237–276.
- Endocrine Society Task Force on Hypoglycemia. Hypoglycemia in Diabetes. Endocr Rev. 2013;34(3):309–338. PubMed
This is educational material for emergency medicine clinicians. It does not constitute medical advice. Always refer to institutional protocols and consult specialists as appropriate for individual patients.
