Last reviewed: March 2026
Contents
MDM Templates
Localized Infection — Erythema Migrans
Patient presents with an expanding annular erythematous lesion consistent with erythema migrans after exposure in an endemic area. They deny heart block symptoms (dizziness, syncope, palpitations), facial nerve palsy, meningismus, or joint swelling. They are well appearing and non-toxic.
Presentation is clinically consistent with localized Lyme disease. Erythema migrans is a clinical diagnosis — serologies are often falsely negative at this stage. History and exam lower suspicion for cellulitis, necrotizing fasciitis, vasculitis, or anaphylaxis.
Plan: Doxycycline 100 mg PO BID x 21 days.
Disposition: Discharge with return precautions for new facial weakness, chest pain, syncope, joint swelling, or worsening neurologic symptoms. PCP follow-up within 1 week.
Early Disseminated Disease
Patient presents with erythema migrans and additional findings consistent with early disseminated Lyme disease — facial nerve palsy / multiple EM lesions / mild cardiac conduction delay (PR interval <300 ms) / arthralgias. They are hemodynamically stable without high-degree AV block.
Presentation is consistent with early disseminated Lyme disease with extracutaneous manifestations. History and exam lower suspicion for idiopathic Bell's palsy, other causes of AV block, or septic arthritis.
Plan: Doxycycline 100 mg PO BID x 21 days (covers both Lyme and potential Anaplasma co-infection).
Disposition: Discharge with close follow-up. Return precautions for syncope, near-syncope, worsening neurologic deficits, or severe headache with meningismus.
Late Lyme / Lyme Carditis
Patient presents with significant AV block (PR >300 ms or high-degree block) in the context of tick exposure history and presentation consistent with Lyme carditis. This warrants admission for IV antibiotics and cardiac monitoring.
Presentation is consistent with Lyme carditis with significant conduction disease. History and exam raise concern for progression to complete heart block.
Plan: Ceftriaxone 2g IV daily. Continuous cardiac monitoring. Temporary pacing equipment at bedside.
Disposition: Admit to telemetry or ICU. Cardiology consultation if high-degree block. Avoid permanent pacemaker placement — Lyme carditis is typically reversible with antibiotics.
Clinical Education
Diagnosis Pearls
Erythema migrans IS the diagnosis. In endemic areas, a classic expanding erythematous lesion >5 cm with central clearing is sufficient to diagnose Lyme and initiate treatment without serologic confirmation. Two-tier testing (ELISA followed by Western blot or second ELISA) is only ~40-60% sensitive during early localized disease because antibodies haven’t developed yet.[1]
The “bull’s-eye” appearance is actually the minority of cases. Homogeneous erythema without central clearing is more common than the classic target lesion. Any expanding erythematous lesion >5 cm after tick exposure in an endemic area should be treated.[1]
Treatment by Stage
| Stage | Treatment | Notes |
| Early localized (EM) | Doxycycline 100 mg PO BID x 21 days | Preferred because it also covers Anaplasma co-infection |
| Early localized (children <8, pregnant) | Amoxicillin 500 mg PO TID x 21 days | Cefuroxime 500 mg BID is an alternative |
| Early disseminated (facial palsy, mild carditis PR <300) | Doxycycline 100 mg PO BID x 21 days | Oral treatment adequate for isolated facial palsy and first-degree block |
| Lyme carditis (high-degree block, PR >300) | Ceftriaxone 2g IV daily x 14-21 days | Admit for monitoring. Conduction abnormalities typically resolve within 1-2 weeks |
| Lyme meningitis | Ceftriaxone 2g IV daily x 14-21 days | Some evidence supports oral doxycycline for Lyme meningitis, but IV remains standard |
| Late Lyme arthritis | Doxycycline 100 mg PO BID x 28 days | Oral treatment is first-line even for arthritis |
Lyme Carditis
Lyme carditis can progress from first-degree to complete heart block rapidly — sometimes within hours. Any patient with Lyme and PR >300 ms, second-degree, or third-degree block needs admission and continuous monitoring. Have transcutaneous pacing pads on the patient.[2]
Avoid permanent pacemaker implantation. Lyme carditis is almost always reversible with appropriate antibiotic therapy. Conduction typically normalizes within 1-2 weeks. Temporary pacing is the bridge if needed.
Atropine may not work because the block in Lyme carditis is often at the level of the His bundle (below vagal innervation), not the AV node. Isoproterenol or temporary pacing may be needed.[2]
Post-Tick Bite Prophylaxis
Single-dose doxycycline 200 mg PO is recommended for prophylaxis when ALL of the following criteria are met: the tick is identified as Ixodes scapularis (deer tick), the tick was attached for >36 hours (engorged), prophylaxis can be given within 72 hours of removal, and the patient is in an endemic area. Do not prophylax for dog ticks or ticks attached <36 hours.[3]
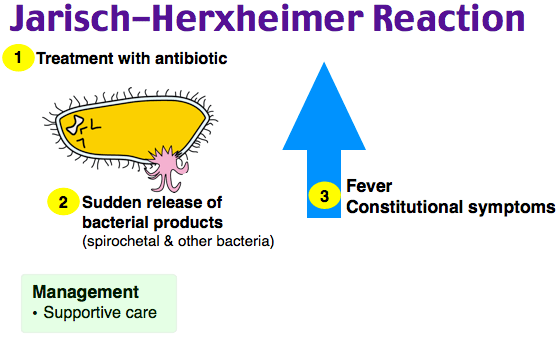
Jarisch-Herxheimer Reaction
Transient worsening of symptoms in the first 24 hours of treatment due to immune response to antigens released from dying spirochetes. Common with treatment of any spirochetal infection (Lyme, syphilis, leptospirosis). Self-limited, managed with NSAIDs and supportive care. Does not warrant antibiotic discontinuation.[1]
References
- Lantos PM et al. Clinical Practice Guidelines by the IDSA, AAN, and ACR: 2020 Guidelines for Prevention, Diagnosis, and Treatment of Lyme Disease. Clin Infect Dis. 2021;72(1):e1-e48. PubMed
- Forrester JD, Mead P. Third-Degree Heart Block Associated with Lyme Carditis: Review of Published Cases. Clin Infect Dis. 2014;59(7):996-1000. PubMed
- Nadelman RB et al. Prophylaxis with Single-Dose Doxycycline for Prevention of Lyme Disease After an Ixodes Tick Bite. N Engl J Med. 2001;345(2):79-84. PubMed
