Last reviewed: March 2026
Contents
MDM Templates
Vaso-Occlusive Crisis — Discharge
Patient with sickle cell disease presents with pain to *** that is consistent with their typical vaso-occlusive crisis pattern. They deny fever, chest pain, dyspnea, hematuria, focal weakness, or confusion. They are afebrile and well appearing.
History and exam lower suspicion for acute chest syndrome, bacteremia, pneumonia, CVA, aplastic crisis, splenic sequestration, osteomyelitis, and renal papillary necrosis. Patient’s pain has been controlled with treatment in the ED.
Plan: Pain management with IV/PO analgesics and IV hydration.
Disposition: Discharge with oral pain medications and return precautions for fever, chest pain, dyspnea, worsening or uncontrolled pain, weakness, or confusion. PCP or hematology follow-up within 48 hours.
Vaso-Occlusive Crisis — Admit
Patient with sickle cell disease presents with severe pain refractory to ED pain management. They are unable to achieve adequate pain control with multiple doses of IV analgesics and require ongoing parenteral pain management.
History and exam lower suspicion for acute chest syndrome, bacteremia, pneumonia, CVA, aplastic crisis, osteomyelitis, and renal papillary necrosis. Despite absence of these complications, pain is refractory to ED management.
Plan: Continued IV hydration and parenteral analgesics. Incentive spirometry to prevent ACS.
Disposition: Admit for intractable pain management and monitoring.
Acute Chest Syndrome
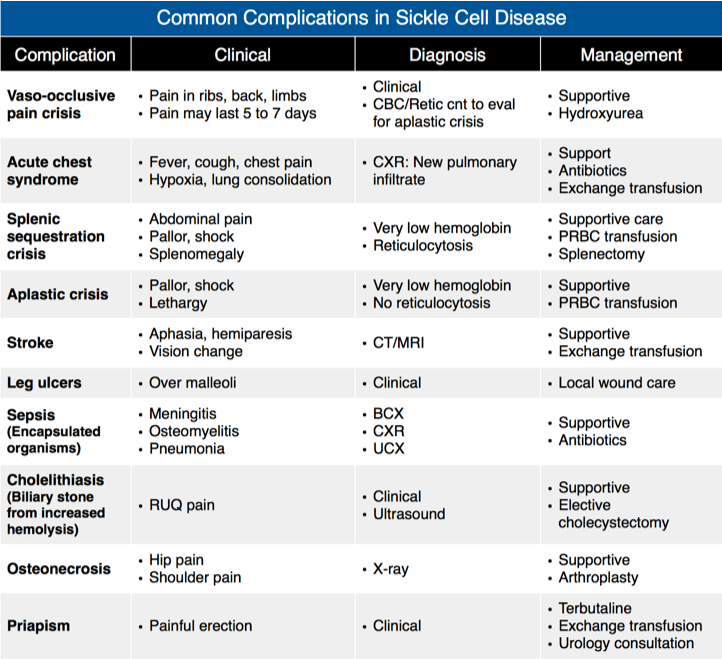
Patient with sickle cell disease presents with fever, cough, chest pain, and dyspnea with new pulmonary infiltrate on imaging. Presentation is consistent with acute chest syndrome, which is the leading cause of death in adults with SCD.
History, exam, and imaging are consistent with ACS. The interplay of pulmonary infection, fat embolism, and in-situ pulmonary vascular sickling makes the distinction between these etiologies academic — management addresses all of them simultaneously.
Plan: Supplemental oxygen, IV hydration (judicious — avoid volume overload), ceftriaxone + azithromycin for atypical coverage, incentive spirometry, pain management. Hematology consulted regarding transfusion versus exchange transfusion.
Disposition: Admit. ICU if rapidly progressive hypoxia, need for exchange transfusion, or hemodynamic instability.
Aplastic Crisis
Patient with sickle cell disease presents with worsening fatigue and pallor. Hemoglobin is significantly below baseline with a markedly depressed reticulocyte count, consistent with aplastic crisis most commonly caused by Parvovirus B19 infection.
The combination of anemia below baseline with low reticulocyte count distinguishes aplastic crisis from hemolytic crisis (which has an elevated reticulocyte count). History and exam raise concern for transfusion-dependent anemia.
Plan: Transfusion to hemoglobin goal per hematology guidance. Hematology consulted. Droplet precautions given Parvovirus B19 risk to pregnant patients and healthcare workers.
Disposition: Admit. Consider IVIG per hematology.
Clinical Education
Pain Management
Treat SCD pain aggressively and without judgment. The 2020 ASH guidelines recommend IV opioids within 30 minutes of triage and reassessment within 15-30 minutes of each dose. Hydromorphone or morphine IV are first-line. Patient-controlled analgesia (PCA) for admitted patients reduces pain scores and provider bias.[1]
Avoid meperidine (Demerol) — it lowers the seizure threshold and accumulates in renal impairment, which is common in SCD. Use ketorolac IV (15-30 mg) as an adjunct, but avoid in renal disease or if there’s concern for GI bleeding.[1]
Fluids: Normal saline at maintenance rate (not aggressive bolusing). Over-hydration can precipitate ACS. Avoid hypotonic fluids in most adults.
Incentive spirometry: 10 breaths every 2 hours while awake. This is one of the most evidence-based interventions to prevent ACS in hospitalized SCD patients.[1]
Acute Chest Syndrome Pearls
ACS = new pulmonary infiltrate + one of: chest pain, fever, cough, dyspnea, or hypoxia. It is a clinical-radiographic diagnosis. Microbiology is most commonly Chlamydia, Mycoplasma, and RSV. Fat embolism from bone marrow infarction is the other major mechanism.[2]
CXR may lag behind clinical deterioration. A patient admitted for vaso-occlusive crisis who develops respiratory symptoms should be treated for ACS even if the initial CXR is clear — repeat imaging in 12-24 hours often shows the infiltrate.
Antibiotics: Ceftriaxone (community-acquired coverage) + azithromycin (atypical coverage) is the standard empiric regimen.
Transfusion Indications
| Indication | Type | Goal |
| Symptomatic anemia (Hgb drop >1 from baseline) | Simple transfusion | Hgb ~10 (do not exceed 10 — hyperviscosity risk) |
| Aplastic crisis | Simple transfusion | Hgb ~10 |
| Acute stroke | Exchange transfusion | HbS <30%. Exchange preferred over tPA. |
| Severe ACS (progressive hypoxia, normal Hgb) | Exchange transfusion | HbS <30% |
| Refractory priapism | Exchange transfusion | After aspiration/phenylephrine fails |
Simple transfusion risk: Adding normal RBCs to a patient with a normal Hgb for SCD (~7-9) can paradoxically worsen sickling by increasing viscosity. Never transfuse past Hgb 10.[3]
Other SCD Complications
Splenic sequestration: Life-threatening. Presents in children age 1-4 (adults with HbSC can get it too) with sudden splenomegaly, falling hemoglobin, and hypovolemic shock. Reticulocyte count is elevated (distinguishing from aplastic crisis). Treat with immediate transfusion (goal Hgb >8) and ICU admission.[3]
Stroke: SCD is the most common cause of childhood stroke. Exchange transfusion is the definitive treatment — preferred over tPA. Simple transfusion to Hgb 10 can be started while awaiting exchange capability.[3]
Osteomyelitis: Salmonella is the most common causative organism in SCD patients (unlike the general population where S. aureus predominates). Any SCD patient with focal bone pain and fever should have osteomyelitis in the differential alongside vaso-occlusive crisis.[3]
References
- Brandow AM et al. American Society of Hematology 2020 Guidelines for Sickle Cell Disease: Management of Acute and Chronic Pain. Blood Adv. 2020;4(12):2656-2701. PubMed
- Vichinsky EP et al. Causes and Outcomes of the Acute Chest Syndrome in Sickle Cell Disease (NHLBI ACS Study). N Engl J Med. 2000;342(25):1855-1865. PubMed
- NHLBI Expert Panel Report. Evidence-Based Management of Sickle Cell Disease. 2014. NHLBI
