Last reviewed: March 2026
Contents
MDM Templates
Distal Radius Fracture
Patient presents with wrist pain and deformity after fall on outstretched hand. Imaging demonstrates distal radius fracture. They do not currently demonstrate complications such as compartment syndrome, neurovascular injury, or open fracture.
Hematoma block performed for analgesia. Fracture reduced and immobilized in sugar tong splint. Post-reduction imaging demonstrates improved alignment. Neurovascular status intact before and after reduction.
Plan: Sugar tong splint. Analgesics. Ice and elevation.
Disposition: Discharge with orthopedic follow-up within 1 week for definitive fracture management. Return precautions for worsening pain, numbness, or inability to move fingers.
If inadequate reduction or operative criteria met:
Orthopedics consulted regarding fracture pattern and need for operative fixation. Criteria for consultation include >5 mm shortening, articular involvement, or >5 degrees dorsal angulation after reduction attempt.
Ulnar Shaft Fracture
Patient presents with forearm pain after injury. Imaging demonstrates ulnar shaft fracture. They do not currently demonstrate complications such as compartment syndrome, neurovascular injury, or open fracture. Wrist and elbow joints stable on exam — no associated radial head dislocation (Monteggia) or DRUJ disruption.
The fracture has been immobilized in a sugar tong splint.
Plan: Sugar tong splint. Analgesics.
Disposition: Discharge with orthopedic follow-up within 1 week. Return precautions for worsening pain, numbness, or swelling.
Scaphoid Fracture
Patient presents with radial-sided wrist pain after fall on outstretched hand. Exam with anatomic snuffbox tenderness and pain with axial loading of the thumb. Imaging does not demonstrate definitive fracture, however clinical exam is concerning for occult scaphoid fracture.
Given high clinical suspicion, the patient is treated presumptively as a scaphoid fracture. Immobilized in a thumb spica splint.
Plan: Thumb spica splint. Analgesics.
Disposition: Discharge with orthopedic follow-up within 1–2 weeks for repeat imaging (X-ray or MRI) to evaluate for occult fracture. Patient counseled on importance of follow-up given risk of avascular necrosis with missed scaphoid fractures.
Procedure Notes
Hematoma Block
Location: *** wrist, fracture site
Time Out: Correct patient, correct procedure confirmed
Approach: Fracture site identified by palpation and imaging. Skin prepped with chlorhexidine in sterile fashion. 18-gauge needle inserted into the fracture hematoma — aspiration of blood confirmed proper needle position
Injection: 10 mL of 1% lidocaine (plain) injected into fracture site
Complications: None. Patient tolerated procedure well with excellent analgesia.
Wrist Fracture Reduction
Location: *** wrist
Time Out: Correct patient, correct procedure confirmed
Consent: Verbal consent obtained
Anesthesia: Hematoma block with 1% lidocaine
Position: Supine
Method: Traction-countertraction technique used to reduce the fracture. Distal fragment disimpacted with longitudinal traction, then volar-directed pressure applied to restore alignment
Post-procedure: Fracture fragments in improved alignment clinically. Post-reduction films confirm improved alignment. Neurovascular status intact before and after reduction
Immobilization: Sugar tong splint applied
Complications: None. Patient tolerated procedure well.
Forearm Nerve Block
Location: *** forearm, *** nerve
Time Out: Correct patient, correct procedure confirmed
Approach: Forearm prepped and cleansed in sterile fashion. *** nerve identified with ultrasound guidance
Injection: 3–5 mL of 1% lidocaine (or 0.25% bupivacaine) injected in the fascial plane surrounding the nerve under direct ultrasound visualization
Complications: None. Patient tolerated procedure well with excellent analgesia.
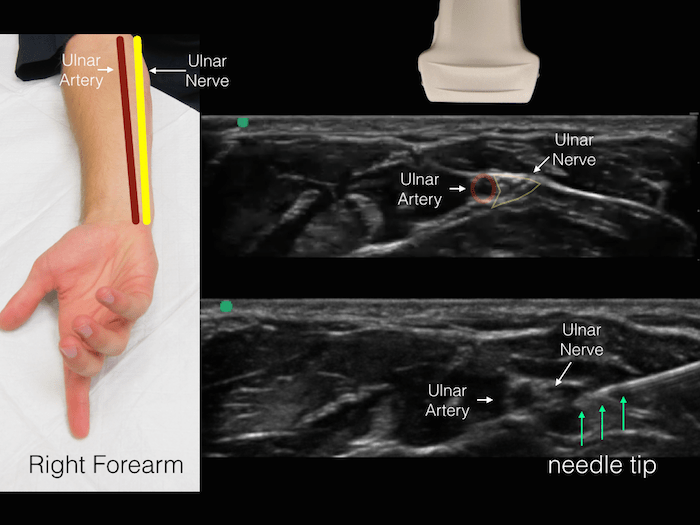
Ultrasound-guided ulnar nerve block
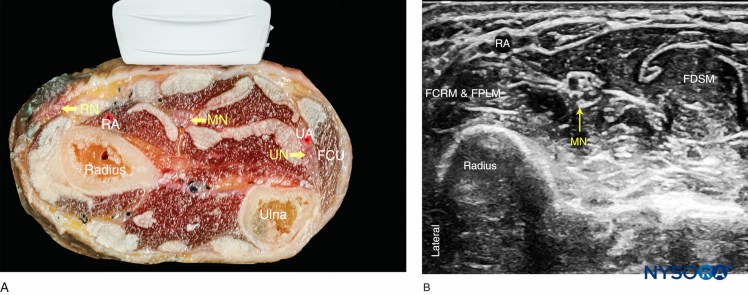
Median nerve anatomy at the wrist
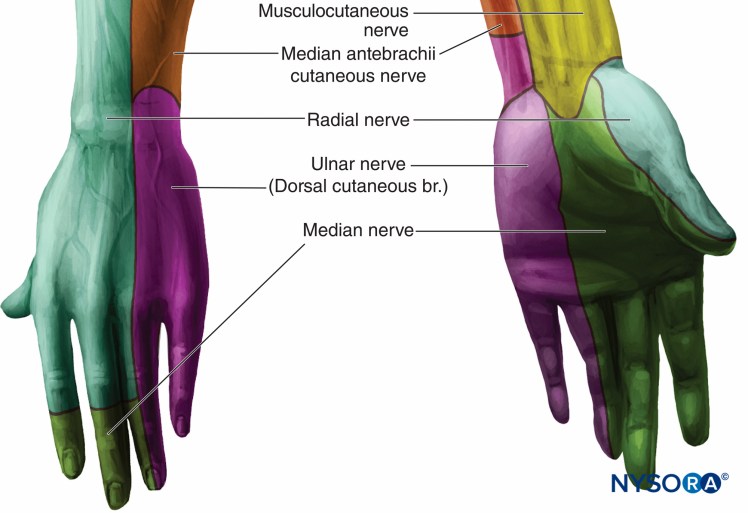
Forearm nerve sensory distributions
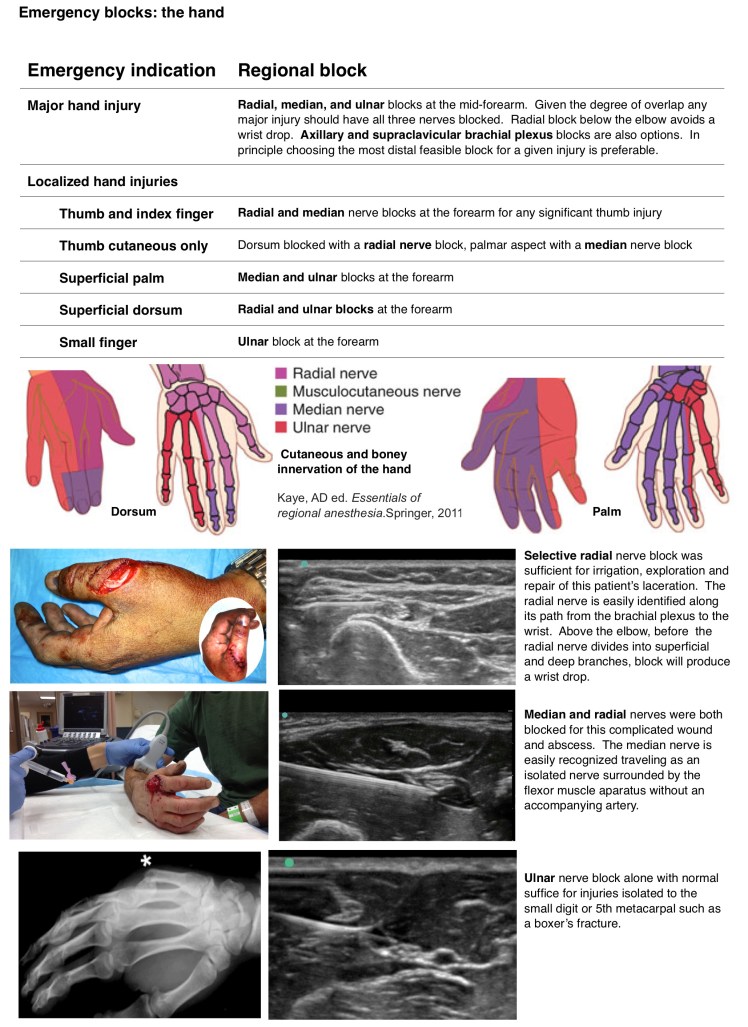
Forearm regional nerve block guide
Clinical Education
Distal Radius Fracture Pearls
Colles fracture (dorsal angulation) is the classic FOOSH injury. Smith fracture (volar angulation) is the reverse — think motorcycle fall or fall onto the back of the hand. The Colles is far more common. Reduction goal: restore radial height, radial inclination, and volar tilt. Post-reduction X-ray should show no more than neutral tilt (0 degrees) — any residual dorsal angulation >5 degrees warrants ortho consultation.[1]
Operative indications: >5 mm radial shortening, intra-articular involvement with >2 mm step-off, >5 degrees dorsal angulation after reduction, or >20 degrees of initial angulation (these tend to re-displace in a splint).
Immobilization: Sugar tong splint is the go-to — it prevents pronation/supination, which is the motion that displaces the fracture. A volar splint alone does not adequately prevent re-displacement.
Both-Bone Forearm Fractures
In adults, both-bone forearm fractures almost always need surgery. The radius and ulna function as a unit — both need anatomic alignment for normal pronation/supination. Splint in sugar tong, keep them comfortable, and consult ortho. In children, closed reduction and casting is more often successful because of remodeling potential.[2]
Scaphoid Fracture Pearls
Initial X-rays are negative in up to 20% of scaphoid fractures. If the patient has anatomic snuffbox tenderness, scaphoid tubercle tenderness, or pain with axial loading of the thumb — treat it as a fracture regardless of X-ray findings. Thumb spica splint and repeat imaging at 10–14 days (X-ray) or obtain an MRI, which can diagnose the fracture immediately.[3]
Why we worry about scaphoid: avascular necrosis. The scaphoid’s blood supply enters distally and flows proximally — proximal pole fractures have the highest AVN risk (up to 30–40%). Displaced fractures (>1 mm) and proximal pole fractures need orthopedic referral for likely surgical fixation. Non-displaced waist fractures can often be managed with casting but need close follow-up.
Galeazzi and Monteggia
These are the “don’t miss” forearm fracture-dislocation patterns. Both need surgical management in adults.[4]
| Pattern | Fracture | Dislocation | Remember |
| Galeazzi | Radial shaft (distal third) | DRUJ disruption | Check the wrist |
| Monteggia | Ulnar shaft (proximal third) | Radial head dislocation | Check the elbow |
Clinical rule: Any isolated forearm bone fracture should prompt you to check the joint above and below. An isolated ulnar shaft fracture → check the elbow for radial head dislocation (Monteggia). An isolated radial shaft fracture → check the wrist for DRUJ disruption (Galeazzi).
Splinting Guide
| Injury | Splint |
| Distal radius / ulna fracture | Sugar tong |
| Scaphoid / thumb base fracture | Thumb spica |
| Forearm shaft fracture | Sugar tong or long arm posterior |
| Nightstick fracture (isolated ulna) | Sugar tong |
Forearm Nerve Block Anatomy
Three nerves supply the hand — blocking all three provides complete anesthesia distal to the wrist. The median nerve lies between palmaris longus and flexor carpi radialis at the wrist (radial side of the forearm). The ulnar nerve runs immediately medial to the ulnar artery. The radial nerve (superficial branch) runs over the radial styloid. Ultrasound-guided blocks at the mid-forearm are more reliable and use less volume than landmark-based approaches at the wrist.[5]
References
- Nellans KW et al. The epidemiology of distal radius fractures. Hand Clin. 2012;28(2):113-125. PubMed
- Jones K, Weiner DS. The management of forearm fractures in children: a plea for conservatism. J Pediatr Orthop. 1999;19(6):811-815. PubMed
- Carpenter CR et al. Adult scaphoid fracture. Acad Emerg Med. 2014;21(2):101-121. PubMed
- Perron AD et al. Orthopedic pitfalls in the ED: Galeazzi and Monteggia fracture-dislocation. Am J Emerg Med. 2001;19(3):225-228. PubMed
- Frenkel O et al. Ultrasound-guided forearm nerve blocks in kids: a novel method for pain management. Pediatr Emerg Care. 2016;32(5):340-342. PubMed
