Last reviewed: March 2026
Contents
MDM Templates
Orbital Wall Fracture
Patient presents with periorbital swelling and pain after blunt facial trauma. CT demonstrates orbital wall fracture. Visual acuity grossly intact. Extraocular movements tested — no restriction or diplopia. Pupils equal and reactive. No enophthalmos. No signs of globe rupture or hyphema on exam.
History and exam lower suspicion for globe rupture, retrobulbar hematoma, muscle entrapment, and intracranial injury.
Plan: Sinus precautions (no nose blowing). Prophylactic antibiotics given communication with sinus tracts. Ice and elevation.
Disposition: Discharge with ophthalmology follow-up within 1 week for dilated retinal exam (blowout fractures carry high risk for retinal injury) and OMFS follow-up for fracture management. Return precautions for vision changes, worsening diplopia, or increased swelling.
If muscle entrapment suspected (restricted EOM, diplopia, nausea/vomiting with upgaze):
Ophthalmology consulted for forced duction testing. Entrapment may resolve spontaneously — emergent surgery is generally not indicated, and intervention can often wait up to 14 days.
If >50% inferior wall involvement or enophthalmos:
OMFS consulted for possible floor reconstruction to prevent permanent enophthalmos. Cheek numbness (infraorbital nerve involvement) further supports significant inferior wall involvement.
Globe Rupture
Patient presents with eye trauma. Exam findings concerning for globe rupture — irregular pupil, shallow anterior chamber, extrusion of intraocular contents, or severely decreased visual acuity. No pressure applied to the globe. Fox shield placed immediately.
CT orbits obtained with thin axial and coronal cuts to confirm rupture and assess for intraorbital foreign body. Ophthalmology consulted emergently.
Plan: Fox shield (no patch — do not apply pressure). IV quinolone antibiotic for endophthalmitis prophylaxis. Tetanus updated. Antiemetics to prevent Valsalva. NPO for likely operative repair.
Disposition: Admit for emergent ophthalmologic surgical repair. Patient counseled that prognosis for vision is guarded, and the goal of repair is to prevent infection and sympathetic ophthalmia.
Facial Fracture — General
Patient presents with facial pain and swelling after blunt trauma. CT demonstrates facial fracture. Airway patent and protected. Cervical spine cleared. No signs of intracranial injury. Dental occlusion intact.
OMFS consulted regarding fracture pattern, need for operative fixation, and timing of repair.
Plan: Analgesics. Soft diet. Sinus precautions if paranasal sinuses involved.
Disposition: Per OMFS recommendation — most isolated facial fractures can be discharged with follow-up within 1–2 weeks for definitive repair planning.
Clinical Education
Orbital Fracture Pearls
Every eye trauma patient deserves a prompt dilated retinal exam. If someone has a blowout fracture, their chance of concurrent retinal injury is high. Even if the ED exam looks fine, arrange ophthalmology follow-up for a dilated exam within 1 week. In the ED, check visual acuity, pupil reactivity (relative afferent pupillary defect suggests optic nerve injury), extraocular movements, and intraocular pressure if globe rupture is not suspected.[1]
If you can’t open the lids to assess EOM: The patient needs ophthalmology for forced duction testing to rule out muscle entrapment before discharge. If entrapment is present and ophthalmology isn’t available, the patient may need transfer.
Diplopia from orbital fracture can be caused by fat entrapment, muscle entrapment, or edema/hemorrhage around the muscle. Fat entrapment and edema often resolve without intervention. True muscle entrapment (inability to move the eye past midline with forced duction) may need surgical release, but this is rarely a same-day emergency.
White-Eyed Blowout
This is the exception that needs urgent surgery. A white-eyed blowout is an orbital floor fracture with inferior rectus muscle entrapment in a patient with a normal-looking eye (no swelling, no bruising — hence “white eye”). Most common in children. The pathognomonic finding is severe nausea and vomiting with attempted upgaze (oculocardiac reflex from muscle traction). These patients need surgical release within 24–48 hours to prevent permanent muscle ischemia and diplopia.[2]
Globe Rupture Pearls
Stop examining the eye the moment you suspect globe rupture. Do not check intraocular pressure, do not force the lids open, do not apply any pressure. Place a Fox shield (rigid eye shield — NOT a patch) and call ophthalmology. Seidel test (fluorescein streaming from a wound site) can confirm a corneal or scleral laceration but should only be done gently and only if the diagnosis is uncertain.[3]
CT findings of globe rupture: irregular globe contour, intraocular air, flat anterior chamber, lens dislocation, or intraocular foreign body. CT has ~75% sensitivity for globe rupture — a negative CT does not rule it out if clinical suspicion is high.
Sympathetic ophthalmia: a rare but devastating autoimmune uveitis in the uninjured eye that can occur days to months after penetrating trauma to the other eye. This is the reason ophthalmology sometimes considers enucleation of a non-salvageable globe. Patient should be warned about new visual symptoms in the uninjured eye.
When to Wake Up Ophthalmology
Call emergently for: significant visual acuity loss, visual field cut (suggests retinal detachment), globe that doesn’t appear anatomically correct (rupture, proptosis), gross orbital abnormalities or telecanthus (widening between medial canthi — suggests naso-orbital-ethmoid fracture with possible globe or lacrimal injury), large hyphema, and elevated intraocular pressure not responding to treatment (may need anterior chamber washout).[4]
Facial Laceration Nerve Blocks
Three blocks cover most of the face. The supraorbital nerve (above the eye), infraorbital nerve (cheek and upper lip), and mental nerve (lower lip and chin) provide regional anesthesia for laceration repair in their respective distributions. All three exit through foramina that line up vertically in the mid-pupillary line. Use 1–2% lidocaine with epinephrine. Onset is rapid and duration is 1–2 hours — plenty for most laceration repairs.
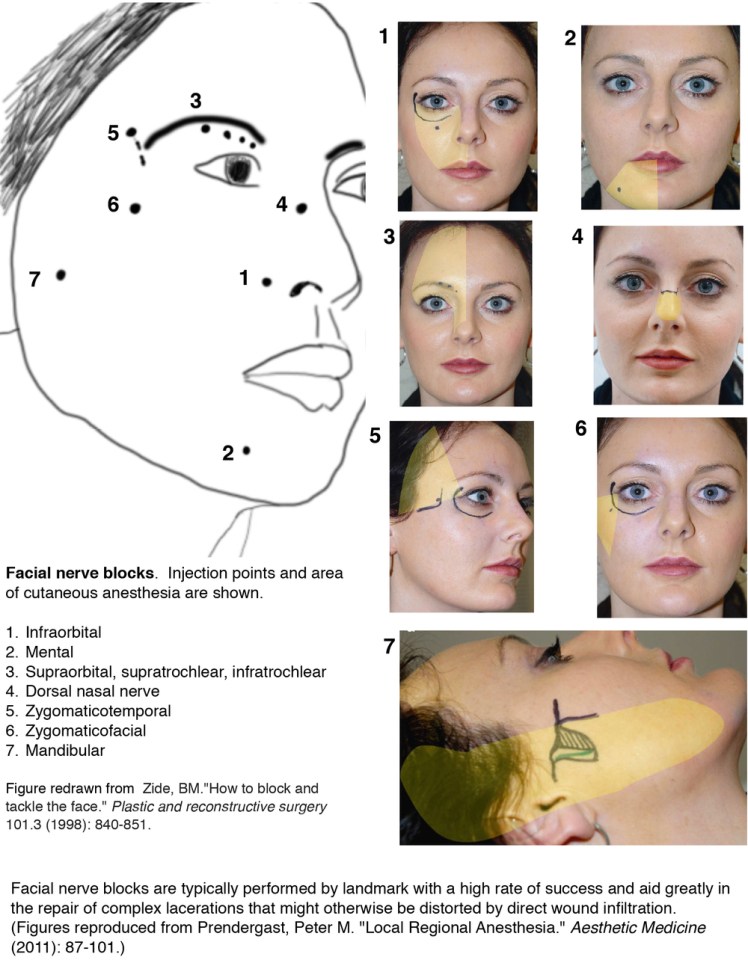
Facial laceration nerve block guide — supraorbital, infraorbital, and mental nerve blocks
References
- Boyette JR, Pemberton JD, Bonilla-Velez J. Management of orbital fractures: challenges and solutions. Clin Ophthalmol. 2015;9:2127-2137. PubMed
- Jordan DR et al. Intervention within days for some orbital floor fractures: the white-eyed blowout. Ophthal Plast Reconstr Surg. 1998;14(6):379-390. PubMed
- Bord SP, Linden J. Trauma to the globe and orbit. Emerg Med Clin North Am. 2008;26(1):97-123. PubMed
- Pokhrel PK, Loftus SA. Ocular emergencies. Am Fam Physician. 2007;76(6):829-836. PubMed
