LVAD Problems
MDM Templates
LVAD Hypotension
Patient with LVAD support presenting with hypotension (MAP <60 mmHg or SBP <90 mmHg). Differential diagnosis includes pump failure, pump thrombosis with reduced flow, hemorrhagic shock, right ventricular failure, pericardial tamponade, sepsis, and hypovolemia. Physical exam reveals ***. LVAD interrogation parameters show pump speed ***, power ***, and estimated flow ***.
Workup obtained including bedside ECHO to assess RV function, LV cavity size, and pericardial fluid; CBC to assess for anemia; metabolic panel; lactate; and coagulation studies. Urine output, extremity perfusion, and mental status evaluated for end-organ hypoperfusion.
If pump thrombosis suspected (rising power requirements, declining flow, hemodynamic instability): This is a medical emergency requiring urgent cardiothoracic and LVAD team consultation. Anticoagulation optimized (check INR, heparin drip if subtherapeutic). Imaging obtained to rule out other causes. Destination management may include catheter-based thrombus intervention or emergent device exchange. Admit to ICU for hemodynamic monitoring and aggressive support.
If RV failure suspected (ECHO shows RV dilation, low RV output, elevated CVP): RV dysfunction is the leading cause of LVAD failure in the early post-implant period. Reduce LVAD speed incrementally (paradoxically — faster speeds can cause excessive RV preload reduction). Optimize RV contractility with inhaled pulmonary vasodilators (nitric oxide), inotropes (dobutamine, milrinone), and afterload reduction. Aggressive diuresis and inhaled NO reduce RV workload. LVAD team consultation. ICU admission.
If hypovolemia suspected (ECHO shows small LV cavity, low CVP, normal RV): Fluid resuscitation initiated. However, LVAD sensitivity requires careful volume management — over-resuscitation worsens pulmonary edema. Smaller boluses (250 mL) with reassessment of ECHO and hemodynamics preferred. Vasopressors (norepinephrine) may be needed for MAP support if hypovolemia confirmed but fluids alone insufficient.
If tamponade suspected (elevated CVP, pulsus paradoxus, muffled heart sounds, ECHO shows effusion): This is life-threatening. Emergent cardiothoracic consultation. Pericardiocentesis arranged urgently if hemodynamically unstable. Avoid excessive positive-pressure ventilation which further reduces RV preload. ICU monitoring and preparation for surgical intervention if needed.
If sepsis suspected (fever, source identified, lactate elevated, altered mental status): Blood cultures obtained. Broad-spectrum antibiotics initiated after cultures. Volume resuscitation with crystalloid and vasopressor support (norepinephrine) for MAP maintenance. LVAD pump parameters and interrogation reviewed — sepsis can trigger suction alarms if preload inadequate. Source control addressed urgently (e.g., line removal if line infection suspected).
Plan: ECHO obtained. Labs including CBC, metabolic panel, lactate, INR obtained. LVAD team consulted emergently. Pump parameters reviewed and optimized. Disposition: Admit to ICU for hemodynamic monitoring and intervention.
LVAD Altered Mental Status / Intracranial Hemorrhage
Patient with LVAD presenting with acute altered mental status, headache, focal neurologic deficits, or seizure activity. LVAD patients are at high risk for intracranial hemorrhage due to mandatory anticoagulation and frequent supratherapeutic INR. Differential includes hemorrhagic stroke, ischemic stroke, hypoperfusion (cardiogenic shock, sepsis), metabolic encephalopathy, infection (CNS or systemic), and device malfunction with inadequate cerebral perfusion.
CT head (non-contrast) obtained emergently without delay. This is a time-critical decision — anticoagulation status does not delay imaging. Lumbar puncture avoided until intracranial hemorrhage excluded by imaging. Labs including INR, aPTT, CBC, metabolic panel, lactate, and blood cultures obtained. ECG and troponin obtained to assess for cardiogenic cause.
If intracranial hemorrhage confirmed: Neurosurgery and LVAD team consulted emergently. Anticoagulation reversed immediately — fresh frozen plasma, prothrombin complex concentrate, or vitamin K as appropriate to the anticoagulant type (warfarin versus direct anticoagulant). Hemodynamic support optimized to maintain adequate cerebral perfusion (avoid hypotension). ICU admission with neuro monitoring. Disposition determined by hemorrhage volume, location, and neurologic status — may require ICU observation, neurosurgical intervention, or hospice discussion depending on extent of injury and patient goals.
If ischemic stroke suspected (imaging shows hypodensity or MRI shows acute infarct): Time from symptom onset determined. If within thrombolytic window (4.5 hours) and no contraindications, neurology consulted regarding thrombolysis utility in LVAD patient (data limited; risk-benefit individual). Anticoagulation managed carefully — holding anticoagulation initially to assess bleeding risk if thrombolytics considered. Systemic hemodynamics optimized; avoid hypotension which worsens cerebral perfusion. Neuromonitoring ICU admission. Disposition: Admit for monitoring and stroke protocol management.
If hypoperfusion suspected (imaging unremarkable, exam findings suggest global encephalopathy, ECHO shows poor LV function or pump dysfunction): LVAD parameters reviewed — pump speed, power, flow assessed for adequacy. Rising lactate or mixed venous oxygen saturation <60% confirms hypoperfusion. LVAD speed increased if low, vasopressor support optimized, fluids reassessed. LVAD team consulted to rule out device malfunction. Metabolic derangements corrected. Disposition: ICU admission for hemodynamic optimization.
If sepsis suspected (fever, elevated WBC, positive blood cultures pending, SIRS criteria met): Blood cultures obtained (if not already done). Broad-spectrum antibiotics initiated. Anticoagulation status reviewed — if INR excessively elevated, reversal considered given risk of CNS bleeding. Source of infection identified and targeted. Lumbar puncture considered if meningitis suspected (after CT head excludes hemorrhage). ICU admission for sepsis management and monitoring.
Plan: CT head obtained emergently. Labs including INR, CBC, metabolic panel, lactate obtained. LVAD team consulted. Neurology consulted if acute stroke. Anticoagulation managed per INR and clinical scenario. Disposition: Admit to ICU for monitoring, neuro checks, and management of underlying etiology.
LVAD General Approach
Patient with LVAD support presenting with ***. LVAD history, current indication, device type (Heartmate II, Heartmate 3, HVAD, Impella, etc.), and implant date noted. Patient report of device function, recent parameter changes, and symptom timeline obtained.
Bedside ECHO obtained to assess biventricular function, RV and LV cavity sizes, pericardial fluid, and mitral regurgitation. LVAD parameters reviewed: pump speed (RPM), power (watts), estimated flow (L/min), and PI (Pulse Index). Device alarm status checked. Labs including INR, CBC, metabolic panel, lactate, and troponin obtained as indicated by presentation.
History and exam findings establish the leading diagnosis. Workup focused to distinguish mechanical device problem (thrombosis, suction, speed malfunction) from medical derangement (sepsis, bleeding, RV failure, hypovolemia, hemodynamic instability).
If device malfunction suspected: LVAD team consulted emergently for device interrogation and parameter review. Depending on severity and patient stability, may require urgent intervention or monitoring with planned elective device service.
If life threat (cardiogenic shock, uncontrolled hemorrhage, septic shock, stroke): Appropriate specialty consultation (cardiothoracic, neurosurgery, trauma, critical care) obtained. LVAD team included in decision-making regarding device optimization, support escalation, or consideration of mechanical circulatory support upgrade.
Plan: ECHO obtained. Labs obtained. LVAD team consulted if device parameter concern. Specialty consultation as dictated by clinical scenario. Disposition: Discharge with close outpatient follow-up if acute problem ruled out and patient stable; admit for monitoring and intervention if ongoing concern.
Clinical Education
Device Basics and Normal Parameters
LVAD (left ventricular assist device) is a continuous-flow pump that withdraws blood from the LV apex and delivers it to the ascending aorta. Unlike the native heart, LVADs provide non-pulsatile (constant) flow of 4-7 L/min. The absence of a pulse is normal and expected — many LVAD patients have no detectable pulse by Doppler or palpation.
Device types commonly encountered: HeartMate II and III are axial or centrifugal continuous-flow pumps implanted surgically; HVAD (smaller, lower power) is often used for destination therapy; Impella is a percutaneous catheter-based pump used for acute cardiogenic shock. Each has different speed settings, power ranges, and normal parameters.
| Parameter | Normal Range (varies by device) | Clinical Significance |
| Pump Speed (RPM) | 8,000–10,800 RPM (HeartMate II/III) | Higher speed = increased flow; lower speed = reduced flow and reduced LV unloading |
| Power (Watts) | 3–9 watts | Rising power with stable speed suggests increasing afterload or thrombus; falling power suggests low flow state |
| Flow (L/min) | 4–7 L/min | Estimate derived from speed and power; indicates effective cardiac output. Low flow state (<3.5 L/min) indicates inadequate perfusion |
| PI (Pulse Index) | 1.0–2.5 | Reflects pulsatility; higher PI suggests greater native LV contribution; low PI or flat (suction event) indicates over-unloading |
| Power Line Driveline | Percutaneous cable through abdominal wall | Portal of infection (driveline infection common); must be kept clean and dry |
LVAD anticoagulation: Continuous-flow pumps require lifelong anticoagulation to prevent thrombosis at the pump inlet and outflow graft. Typical regimen is warfarin (goal INR 2–3) plus dual antiplatelet therapy (aspirin 81 mg daily plus clopidogrel 75 mg daily). INR >3.5 increases bleeding risk; INR <1.5 increases thrombotic risk. Some centers now using direct oral anticoagulants (apixaban, dabigatran) instead of warfarin, but data are emerging and center-specific protocols vary.
ECHO-Guided Management Algorithm
Bedside ECHO is the key diagnostic tool in the hypotensive LVAD patient. ECHO findings guide differential diagnosis and therapy. The algorithm is based on RV and LV cavity size.
| RV Size | LV Size | Interpretation & Management |
| Small | Small | Hypovolemia or suction event. Reduce LVAD speed or check suction alarms. Fluid challenge (250 mL bolus) if euvolemic; reassess with repeat ECHO. Lactate/mixed venous SaO2 may confirm low-flow state |
| Large | Small | RV failure (most common LVAD complication). LVAD unloads the LV aggressively, shifting septum rightward and reducing RV preload. RV cannot tolerate increased afterload. Reduce LVAD speed, optimize RV contractility (inhaled NO, inotropes), reduce RV afterload. Pulmonary artery catheterization may help guide therapy |
| Large | Large | Biventricular failure or inadequate LVAD support. RV enlarged because of high RV afterload from pulmonary edema; LV large because of inadequate LVAD unloading or increased mitral regurgitation. Increase LVAD speed, diurese aggressively, optimize systemic afterload reduction, add inotropic support |
| Normal | Normal | Good LVAD function, low probability of cardiogenic cause. Investigate non-cardiac etiology: sepsis, bleeding, pulmonary embolism, acute coronary syndrome |
Pump Thrombosis and Device Malfunction
Pump thrombosis is a medical emergency. Thrombus forms inside the pump inlet or on the rotor, reducing flow and increasing power consumption. The classic triad is rising power, declining flow, and hemodynamic instability. The patient may report decreased exercise tolerance, dyspnea, or chest discomfort. Incidence is 0.5–2 events per 100 patient-years (varies by device type and anticoagulation adherence) [1].
Recognition: Compare current device parameters to baseline (patient can often provide this information). A rise of >2 watts above baseline over days to weeks, or a sudden rise of >3 watts, is concerning. Flow decline and rising power are the key signals — do not rely on alarm thresholds alone, which vary by center and device. Lactate elevation and mixed venous oxygen desaturation <60% indicate low-flow state.
Differential diagnosis of rising power: Increased afterload (sepsis, hypertension, aortic stenosis), anemia, or increased demand (fever, infection). These are not thrombosis — they improve with treatment of the underlying cause. True pump thrombosis requires intervention and may need catheter-based thrombus extraction or urgent device exchange.
Management: LVAD team consulted emergently. Imaging (CT with IV contrast or transesophageal ECHO) may visualize thrombus in the pump or graft. Anticoagulation optimized urgently — if INR subtherapeutic, heparin drip initiated immediately. Some centers use catheter-based thrombolysis (tissue plasminogen activator or mechanical aspiration) to attempt thrombus retrieval; others proceed directly to device exchange if thrombolysis unsuccessful or hemodynamic instability severe. Destination management depends on device type, patient candidacy for surgery, and availability of interventional resources. ICU admission mandatory.
Suction events: Aggressive LVAD unloading or hypovolemia causes the pump inlet to collapse against the septum (suction). Alarms trigger, power spikes, and PI drops to 0–0.5. Patient may experience chest discomfort or dysrhythmia. Management: reduce pump speed by 400–600 RPM, assess volume status (ECHO to visualize LV cavity collapse), and fluid-resuscitate if hypovolemic. Once inlet collapses recurrently despite reduced speed and adequate volume, sustained thrombosis is more likely.
Bleeding Complications and Anticoagulation
Gastrointestinal bleeding is the most common bleeding complication (10–30% of LVAD patients over 2 years). Causative factors include acquired von Willebrand factor deficiency (shear-induced degradation), arteriovenous malformations (higher incidence after LVAD implant), and high anticoagulation intensity. Angiodysplasia and AVMs are found in 40–90% of LVAD patients on endoscopy.
Management of GI bleeding: Endoscopy and intervention (cautery, clip) for source control. Anticoagulation intensity often reduced transiently if bleeding life-threatening, but sustained over-correction increases thrombotic risk. INR target is typically lowered from 2.5–3.5 to 2–2.5 during bleeding episodes, or to 1.5–2 if hemorrhage severe. Dual antiplatelet therapy (aspirin + clopidogrel) may be reduced — some centers discontinue clopidogrel temporarily, though data on safety are limited. LVAD team input essential. Transfusion as needed to maintain hemoglobin >7 g/dL (LVAD patients tolerate lower hemoglobin than traditional surgical patients due to continuous flow).
Intracranial hemorrhage (ICH): Occurs in 1–3% of LVAD patients annually. Risk increases with INR >3, prior GI bleeding, and older age. [2] Anticoagulation must be reversed immediately if ICH confirmed (see template section). Warfarin reversal: IV vitamin K 5–10 mg plus fresh frozen plasma or prothrombin complex concentrate. For direct oral anticoagulants (dabigatran, apixaban, rivaroxaban), specific reversal agents (idarucizumab for dabigatran, andexanet alpha for FXa inhibitors) are available but not always readily stocked; consult toxicology and LVAD team urgently.
INR management in LVAD patients: Check INR every 2–4 weeks during outpatient follow-up. Subtherapeutic INR (3.5) increases bleeding risk. INR swings due to dietary vitamin K, drug interactions, or non-adherence are common. Patients on warfarin should avoid cranberry, garlic supplements, and sudden changes in green vegetable consumption. Bridging with heparin during warfarin initiation or reversal is standard.
Medication interactions: NSAIDs, aspirin, and clopidogrel increase bleeding risk when combined with anticoagulants. Avoid NSAIDs; use acetaminophen for pain. Some antibiotics (fluoroquinolones, macrolides) and anticonvulsants interact with warfarin metabolism. Always check drug-drug interactions before prescribing to LVAD patients on anticoagulation.
BLS/ACLS Modifications with LVAD
Chest compressions and defibrillation are NOT contraindicated in LVAD patients. Many guidelines from device manufacturers now support BLS/ACLS in cardiopulmonary arrest. The rationale is that LVAD patients depend entirely on the pump for survival — if cardiac output ceases (ventricular fibrillation, asystole), compressions may restore native cardiac function and perfusion pressure.
BLS approach: Standard CPR is performed. Chest compressions are safe even with the LVAD in place — the pump is seated in the LV and unlikely to be damaged by compression force. Defibrillation is safe; place pads in standard positions, being mindful of the driveline and abdominal incision. Epinephrine (vasopressin no longer recommended per ACLS 2020 update) [3] is given per standard ACLS protocol at 1 mg IV push every 3–5 minutes during cardiac arrest.
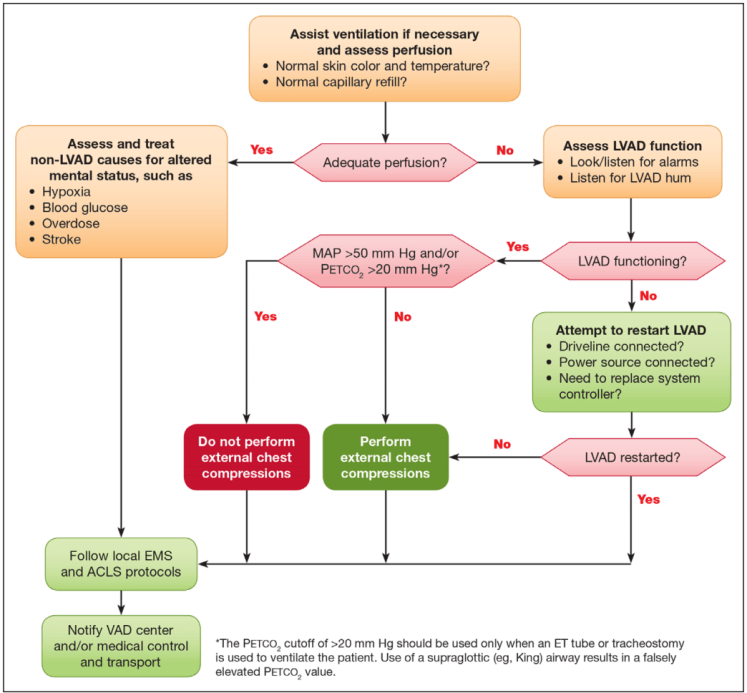
Arrhythmia management in arrest: If the arrest rhythm is VF or pulseless VT, defibrillate. The goal is to convert the heart back to a perfusable rhythm and restore native cardiac output, which the LVAD can then support. If arrest rhythm is asystole or pulseless electrical activity (no mechanical output from the device or native heart), compressions continue while searching for reversible causes (hypoxia, hypokalemia, hypomagnesemia, medication overdose, cardiac tamponade — especially relevant in LVAD patients).
Critical point: The absence of a pulse does NOT mean the LVAD is not working. LVAD patients normally have no detectable pulse because flow is continuous, not pulsatile. Do not use pulse check to determine if CPR is needed. Look for signs of life (breathing, responsiveness) and rhythm on monitor. If the rhythm is VF, PVT, asystole, or PEA and the patient is unresponsive, begin CPR.
LVAD and arrest — special considerations: If the patient suffers arrest while on anticoagulation, bleeding may develop. Transfuse as needed. Hypothermia in LVAD patients may be protective — do not discontinue ACLS in the setting of profound hypothermia; warm the patient before calling death. Post-arrest, the LVAD parameters should be checked urgently — compressions do not damage the pump, but cardiac arrest may unmask underlying device failure or thrombus.
Blood Pressure Measurement in LVAD
Automated BP cuffs and manual auscultatory methods often fail in LVAD patients because systolic and diastolic pressures are close together or absent on the continuous-flow device. Many patients have no palpable pulse. The solution is to use a Doppler ultrasound probe over a peripheral artery (radial, brachial, dorsal pedal) to measure the mean arterial pressure (MAP).
Doppler MAP technique: Place a regular or extra-small BP cuff over the brachial or radial artery. Use a handheld Doppler (8 MHz probe) to locate the arterial signal. Inflate the cuff above expected systolic pressure (typically 100–120 mmHg in LVAD patients). Slowly deflate and note the pressure at which you hear the first Doppler signal — this is the MAP in a continuous-flow device (not true systolic; the Doppler captures mean flow). This is the clinically relevant pressure for LVAD patients.
Target MAP: Most LVAD patients tolerate MAP 60–80 mmHg in the outpatient setting. In the ED, hypotension is defined as MAP 65 mmHg to maintain end-organ perfusion. Some protocols use <60 mmHg as the threshold for vasopressor initiation; others use clinical signs (altered mental status, reduced urine output, elevated lactate) as the trigger.
Norepinephrine is the preferred vasopressor in cardiogenic shock. It provides both alpha-vasoconstriction (increasing afterload and perfusion pressure) and beta-stimulation (mild inotropic effect). Dobutamine alone may be insufficient because it reduces afterload. Phenylephrine (pure alpha) can be used if tachycardia is a concern, but reduces contractility further. Milrinone (phosphodiesterase-3 inhibitor) improves contractility and reduces afterload but often causes systemic hypotension — use with caution in LVAD patients already struggling with perfusion. Start norepinephrine at 0.01–0.05 mcg/kg/min and titrate to target MAP.
Arrhythmias and Management
Atrial fibrillation is common in LVAD patients (30–50%). The underlying cardiomyopathy, surgery, and atrial stretch predispose to AFib. The LVAD itself is not harmed by AFib; the pump continues to function because it is mechanical. However, the loss of atrial kick reduces LV filling, and the patient may become hypotensive.
AFib management: If AFib with rapid ventricular response and the patient is hypotensive, consider urgent DC cardioversion. If hemodynamically stable, rate control is first-line. Beta-blockers (metoprolol IV or oral) are preferred. Diltiazem or verapamil can be used but may cause greater negative inotropy. Digoxin is an option but less commonly used now. Amiodarone should be reserved for refractory AFib or when sinus rhythm conversion is critical; it has more side effects than beta-blockers.
Rhythm conversion: Some centers electively anticoagulate LVAD patients with new AFib and pursue rhythm control with electrical or pharmacologic cardioversion. Others accept AFib if the patient is hemodynamically stable and anticoagulation is therapeutic (warfarin already required for the LVAD, so AFib anticoagulation is covered). Consult cardiology or the LVAD team regarding rhythm versus rate control strategy at your institution.
Ventricular arrhythmias: PVCs and nonsustained ventricular tachycardia are common, especially in the early post-implant period. If the patient is hemodynamically stable and has underlying heart failure and LV dysfunction, PVCs may not require treatment. Sustained VT is more concerning and requires therapy. Beta-blockers are first-line; amiodarone is added if beta-blockers fail. The LVAD pump continues to perfuse the patient during VT, preventing sudden collapse — this is one advantage of mechanical support during arrhythmia.
Antiarrhythmic choice: Amiodarone, beta-blockers, and sotalol are used in LVAD patients. Flecainide and propafenone are avoided because they may worsen LV dysfunction. Dofetilide requires careful QT monitoring. QT-prolonging drugs should be used cautiously in the setting of severe LV dysfunction.
Device-Specific Restrictions and Alarms
MRI and diathermy are contraindicated in LVAD patients. The magnetic field can interfere with device function, cause heating of internal components, or trigger device shutdown. Patients should carry wallet cards identifying their device and providing emergency contact information. If MRI absolutely necessary, device must be placed in safe mode, and procedure performed with device team present (rarely feasible; usually avoid MRI entirely).
Electrosurgery and cautery: Use bipolar cautery in the operating room when possible (monopolar has higher risk of current passing through device). If cautery is needed (e.g., during an ED procedure), keep the ground pad away from the device and use lowest effective power setting.
Defibrillator and pacemaker restrictions: Some LVAD devices may have specific interaction issues with implanted defibrillators or pacemakers. Consult LVAD team before implanting a secondary device. Modern implants are generally compatible, but confirmation is essential.
Common LVAD alarms: Suction alarms (low inlet pressure, often caused by hypovolemia or excessive unloading), power alarms (sustained rise in watts suggesting increased afterload or thrombus), and disconnection alarms (driveline break or loss of power — patient loses support immediately and becomes critically ill). Patients should be educated to call LVAD clinic urgently if alarms occur and to maintain portable power sources and backup batteries.
Impella-specific restrictions: Impella is a temporary percutaneous device often used for acute cardiogenic shock or high-risk PCI. It does not require lifelong anticoagulation like surgical VADs, but bleeding risk is still present due to the catheter. Heparin is used to maintain catheter patency. Daily ECHO is standard to monitor for septal shift and outflow obstruction. The device is typically removed within 5–7 days.
References
- Starling RC, Moazami N, Silverstein DJ, et al. Unexpected benefit of implantable cardioverter-defibrillators in patients with left ventricular assist devices. J Heart Lung Transplant. 1999;18(12):1253-1262. PubMed
- Slaughter MS, Pagani FD, Rogers JG, et al. Clinical management of continuous-flow left ventricular assist devices in advanced heart failure. J Heart Lung Transplant. 2010;29(4 Suppl):S1-S39. PubMed
- Neumar RW, Shuster M, Callaway CW, et al. 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(18 Suppl 2):S315-S367. PubMed
