Last reviewed: March 2026
Contents
MDM Templates
Finger Dislocation
Patient presents with *** finger deformity after injury. *** hand dominant. Dislocation of the *** PIP joint successfully reduced at bedside. Neurovascular exam intact before and after reduction. No rotational deformity. Joint stable through range of motion.
History and exam not consistent with fracture, tendon injury, or neurovascular compromise. The dislocation has been satisfactorily reduced and immobilized.
Plan: Buddy taping. Analgesics.
Disposition: Discharge with return precautions and follow-up within 1 week.
Distal Finger Amputation
*** hand dominant patient presents with distal finger amputation of ***. No apparent flexor or extensor tendon involvement. Neurovascular status of remaining digit assessed.
If revision amputation / primary closure:
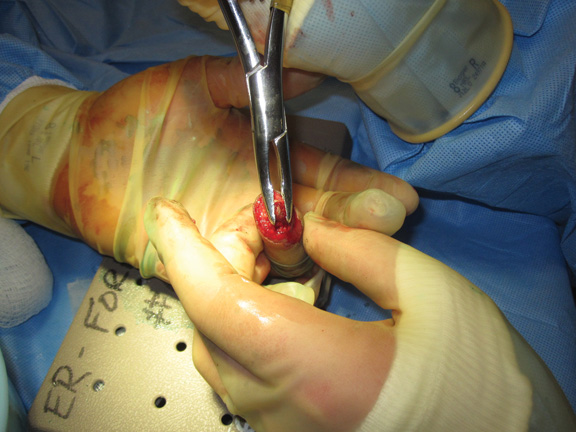
Digital block performed. Wound irrigated. Bone rongeured to allow primary skin closure. No tendon involvement. Wound closed primarily.
Plan: Prophylactic antibiotics. Wound care instructions.
Disposition: Discharge with 48-hour wound check and hand surgery follow-up within 1 week.
If replantation considered (thumb, multiple digits, proximal to DIP, pediatric):
Amputated part wrapped in sterile saline-moistened gauze, placed in plastic bag on ice. Hand surgery consulted regarding replantation candidacy. Wound irrigated. Flexor tendon sheath block with 0.25% bupivacaine for analgesia.
Thumb Fracture
Patient presents with thumb pain after injury. *** hand dominant. Imaging demonstrates fracture of the thumb. Neurovascular exam intact distally. No rotational deformity. Compartments soft.
History and exam not consistent with compartment syndrome, neurovascular injury, or open fracture.
Plan: Thumb spica splint. Analgesics.
Disposition: Discharge with hand surgery follow-up within 1 week. Patient understands that operative fixation may be required.
Finger Tendon Injury
Patient presents with a tendon injury to the *** hand that does not require inpatient admission or emergent surgical intervention. *** hand dominant. Neurovascular exam intact. No signs of flexor tenosynovitis or compartment syndrome.
Patient stabilized in the ED with wound care and splinting. They understand that ED care is stabilizing and that operative repair may be required.
Plan: Splint in position of safety. Analgesics.
Disposition: Discharge with orthopedic/hand surgery follow-up within 1 week.
Finger Nerve Injury
Patient presents with a laceration and sensory deficit to the *** consistent with digital nerve injury. Motor and vascular exam intact. No signs of tendon injury or flexor tenosynovitis.
Wound irrigated and closed. Patient stabilized in the ED. They understand that operative nerve repair may be required and that the care provided today is stabilizing, not definitive.
Plan: Wound care. Analgesics.
Disposition: Discharge with hand surgery follow-up within 72 hours for optimal nerve repair timing.
Paronychia
Patient presents with pain, swelling, and fluctuance adjacent to the nail fold consistent with paronychia. No extension to the volar pulp (felon) or tracking along the tendon sheath (flexor tenosynovitis). Well appearing without fever.
History and exam lower suspicion for felon, herpetic whitlow, flexor tenosynovitis, and osteomyelitis.
Plan: Nail fold elevated with blunt instrument for drainage. Warm soaks. Antibiotics deferred given uncomplicated presentation.
Disposition: Discharge with return precautions for worsening redness, swelling, or fever.
Felon
Patient presents with tense, painful swelling of the fingertip pulp consistent with felon. No signs of flexor tenosynovitis, septic arthritis, or osteomyelitis.
Incision and drainage performed. Wound culture sent.
Plan: TMP-SMX for empiric coverage. Wound care with daily warm soaks.
Disposition: Discharge with 48-hour wound check and PCP follow-up. Caller to follow up wound culture.
Herpetic Whitlow
Patient presents with grouped vesicles on an erythematous base involving the distal finger, consistent with herpetic whitlow. No fluctuance to suggest felon or paronychia. No Kanavel signs for flexor tenosynovitis.
History and exam lower suspicion for felon, paronychia, flexor tenosynovitis, and necrotizing soft tissue infection. Incision and drainage is contraindicated — this is a viral process, not an abscess.
Plan: Topical acyclovir 5%. Clean dressings to prevent autoinoculation and spread.
Disposition: Discharge with follow-up within 1 week. Self-limited — resolves in 2–3 weeks.
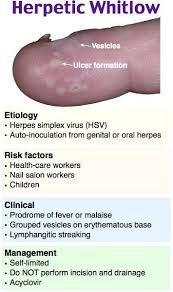

Herpetic whitlow — grouped vesicles, do NOT incise and drain
Procedure Notes
Finger Reduction
Location: *** digit, *** joint, *** hand
Time Out: Correct patient, correct procedure confirmed
Consent: Verbal consent obtained
Anesthesia: Digital block with *** lidocaine
Method: Gentle traction-countertraction technique used to reduce the joint
Post-procedure: Joint appears clinically reduced. Post-reduction films confirm anatomic reduction. Neurovascular status intact before and after reduction. Stable through range of motion
Immobilization: Buddy taping / aluminum finger splint applied
Complications: None. Patient tolerated procedure well.
Clinical Education
Flexor Tendon Zones
Zone 2 (“no man’s land”) is the most technically challenging for repair — both the FDS and FDP run in a tight fibro-osseous tunnel here, and adhesion formation is a major problem. Zone 2 injuries need hand surgery follow-up for operative repair. In the ED, close the skin, splint in position of safety (wrist in slight flexion, MCP joints at 70–90 degrees, IP joints extended), and refer.[1]
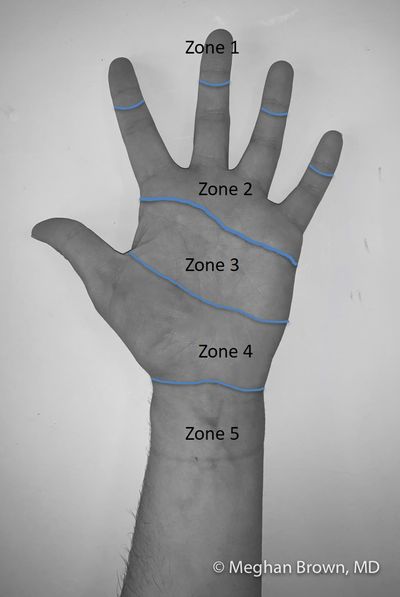
Flexor tendon zones — Zone 1: distal to FDP insertion. Zone 2: A1 pulley to FDP insertion. Zone 3: lumbrical origins.
Test both tendons independently. FDP: hold the PIP joint extended and ask the patient to flex the DIP. FDS: hold all other fingers in extension and ask the patient to flex the PIP of the tested finger.
Nerve Repair Timing
Optimal window for nerve repair is within 72 hours. During this window, the distal nerve ends still contain neurotransmitters, allowing intraoperative motor stimulation for topographical alignment. After 72 hours, edema and scar tissue make exploration and repair technically more difficult. Lacerations causing neurotmesis (complete transection) need operative repair. Crush injuries (axonotmesis) may recover spontaneously over weeks to months. Mild compression/stretch (neuropraxia) self-resolves in days to weeks.[2]
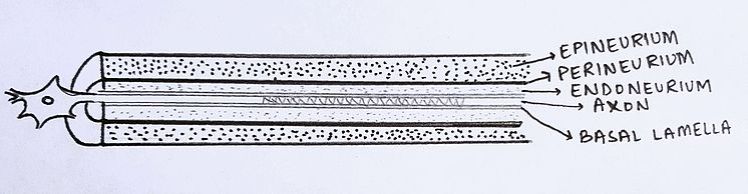
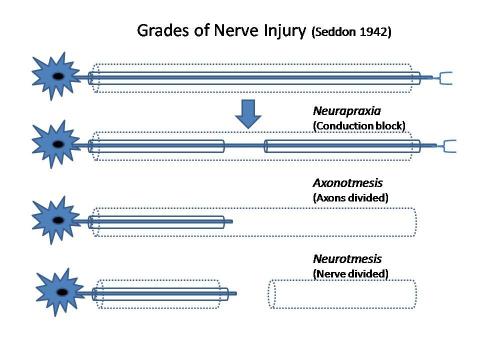
Nerve injury classification: neuropraxia, axonotmesis, neurotmesis
Amputation Pearls
Replantation indications: thumb amputation (most important), multiple digits, amputation proximal to the DIP, and pediatric patients. Amputated parts remain viable for 6–12 hours if properly preserved (saline-moistened gauze in a sealed bag on ice — never place the digit directly on ice). If replantation is indicated and not available at your facility, transfer early.[3]
Single digit amputation distal to the DIP without tendon involvement: revision amputation with rongeur and primary closure is appropriate in the ED. If tendon involvement is present, hand surgery follow-up is mandatory — this patient may need staged reconstruction.
Thumb Fracture Classification
Bennett fracture: intra-articular fracture-dislocation of the thumb CMC joint. A small volar fragment stays attached to the trapezium while the metacarpal shaft displaces proximally and radially. Almost always needs operative fixation (CRPP or ORIF). Rolando fracture: comminuted version of a Bennett’s — even worse prognosis, always surgical.[4]
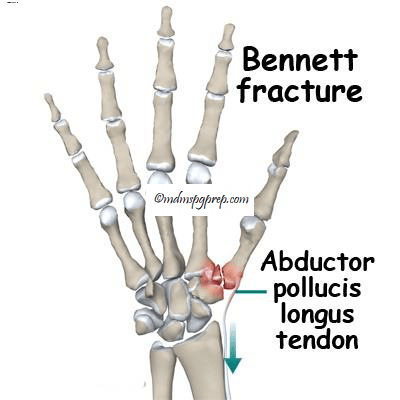
Bennett fracture — intra-articular thumb CMC fracture-dislocation
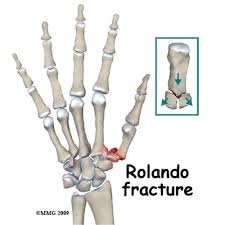
Rolando fracture — comminuted Bennett’s
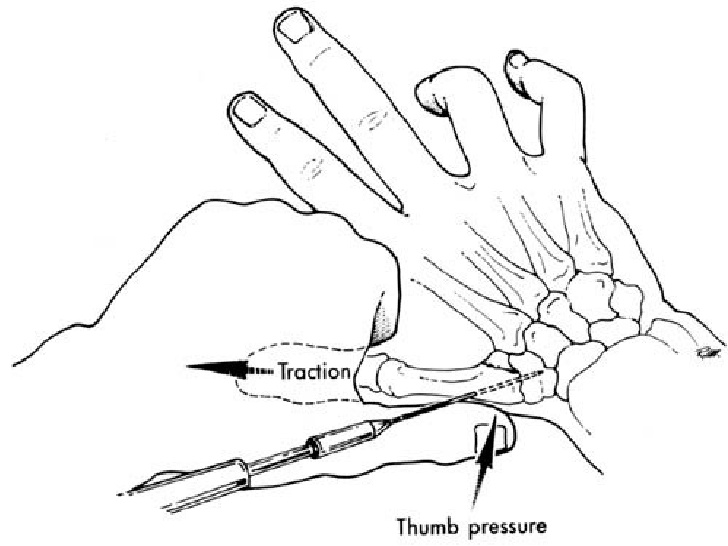
Thumb fracture reduction: longitudinal traction with pressure to thumb base
Extra-articular thumb metacarpal fractures: reduce if >30 degrees angulation. Immobilize in thumb spica. Operative if >30 degrees angulation persists after closed reduction.
Hand Infection Pearls
Paronychia: Lift the nail fold with an 18-gauge needle or #11 blade — no need for full I&D if you can decompress the collection. No antibiotics needed for uncomplicated cases. For chronic/recurrent paronychia, consider fungal etiology (fluconazole 150 mg weekly x 4 weeks) or eczematous etiology (topical steroid).[5]
Felon I&D: Use a longitudinal incision along the area of maximal fluctuance. Avoid fishmouth incisions, through-and-through incisions, and incisions through the flexor crease — all associated with complications including painful scars, neurovascular injury, and unstable finger pad. After drainage, break up the septa with a blunt instrument to ensure complete decompression.
Antibiotic selection for hand infections: TMP-SMX covers MRSA, which is increasingly common. Add cephalexin if significant surrounding cellulitis. For immunocompromised, diabetic, or IVDU patients, consider clindamycin or amoxicillin-clavulanate for broader coverage.
Felon — tense pulp space infection
Flexor Tenosynovitis
Kanavel signs are the clinical diagnosis — all four together are highly specific, but any one should raise concern. The signs are: fusiform (sausage) swelling of the finger, flexed posture of the finger at rest, tenderness along the flexor tendon sheath, and pain with passive extension. This is a surgical emergency — late diagnosis leads to tendon necrosis and a nonfunctional finger.[6]
If you suspect flexor tenosynovitis, consult hand surgery immediately. Early cases (presenting within 24 hours, no systemic toxicity) may be trialed with IV antibiotics and close observation with serial exams. Most need operative irrigation and debridement. Don’t let antibiotics delay surgical consultation.
References
- Strickland JW. Development of flexor tendon surgery: twenty-five years of progress. J Hand Surg Am. 2000;25(2):214-235. PubMed
- Dahlin LB, Wiberg M. Nerve injuries of the upper extremity and hand. EFORT Open Rev. 2017;2(5):158-170. PubMed
- Sears ED, Chung KC. Replantation of finger avulsion injuries: a systematic review of survival and functional outcomes. J Hand Surg Am. 2011;36(4):686-694. PubMed
- Carlsen BT, Moran SL. Thumb trauma: Bennett fractures, Rolando fractures, and ulnar collateral ligament injuries. J Hand Surg Am. 2009;34(5):945-952. PubMed
- Rigopoulos D et al. Treatment of nail disorders. Dermatol Ther. 2002;15(4):369-375. PubMed
- Giladi AM et al. Trends in the management of pyogenic flexor tenosynovitis. Plast Reconstr Surg. 2015;136(1):157-166. PubMed
