Tracheostomy Problems
Last reviewed: March 2026
Quick Links:
MDM Templates
Tracheostomy Bleeding
Patient with established tracheostomy presents with bleeding from the stoma site. Bleeding volume is modest and hemodynamically stable. Patient well-appearing with normal oxygen saturation on current trach settings. History and exam lower suspicion for massive hemorrhage, deep tracheal injury, or tracheo-innominate fistula.
Approach to superficial bleeding: Bleeding localized to stoma margin and cannula site. Direct pressure applied with sterile gauze; bleeding controlled without difficulty. Stoma site cleaned and inspected for granulation tissue, suture irritation, or local infection. If bleeding persists despite direct pressure, topical hemostasis achieved with silver nitrate cautery or application of hemostatic gauze (Surgicel, thrombin-soaked packing). Inner cannula removed, suctioned, and replaced if debris present. Tracheostomy tube cleaned and repositioned to ensure cuff seal without excessive pressure on anterior tracheal wall.
If deep tracheal bleeding suspected: Any bleeding that continues despite local measures, arises from deeper in the stoma (not the cannula-tissue interface), or is accompanied by hemodynamic instability raises concern for tracheal wall injury or vascular erosion. Do not attempt blind control. Call respiratory therapy and anesthesia stat. Position patient sitting upright and leaning forward. Keep suction at bedside. If actively bleeding with hemodynamic compromise, cuff hyperinflated to tamponade bleeding while emergent surgical consultation obtained. Direct the surgical team to consider rigid endoscopy for visualization and control, possible tracheal repair or vessel ligation. Interventional radiology consulted if arterial injury suspected and cuff tamponade achieved.
Plan: If superficial bleeding controlled, continue routine trach care with careful monitoring. If deep bleeding or vascular concern, admit for continuous monitoring, keep NPO, ensure surgical capability available.
Disposition: Mild superficial bleeding may be managed as outpatient if bleeding controlled, patient reliable, and no signs of infection or injury. Any concern for deep tracheal injury or vascular erosion requires hospital admission for observation, possible endoscopy, and surgical standby. Return precautions: any recurrent bleeding, hemodynamic instability, difficulty breathing around or through the trach, or signs of infection warrant immediate evaluation.
Tracheostomy Displacement / Decannulation
Patient with tracheostomy presents with accidental dislodgement or removal of the tracheostomy tube. Timing since tracheostomy placement is critical in determining management approach.
Fresh tracheostomy (< 7 days since placement): Tract is immature and has not epithelialized. Do NOT attempt blind replacement through the stoma — there is high risk of false passage creation, which will result in subcutaneous placement and complete loss of the airway. Instead, immediately call anesthesia and prepare for oral intubation. Patient placed on high-flow oxygen by face mask. If patient in severe distress, may gently attempt single pass with bougie through stoma to guide a 6.0 cuffed ETT into the stoma, but this should only be attempted by experienced personnel if oral intubation is not rapidly available. Standard management is oral intubation via direct laryngoscopy, which is reliable and does not risk false passage. Tracheostomy tube NOT replaced acutely; tract allowed to mature under observation.
Mature tracheostomy (> 7 days since placement): Tract is epithelialized and established. Replacement through the stoma is safe. Tracheostomy tube reinserted over a bougie or using a 6.0 cuffed ETT as a guide. After tube placed, cuff inflated, tube secured, and breath sounds confirmed over bilateral lung fields. Chest imaging (chest X-ray or portable) obtained to confirm tube position (should be at the level of the carina, 2-3 cm above the carina). Patient reassessed for stable oxygen saturation and no subcutaneous emphysema.
Plan: If fresh trach, secure airway via oral intubation and monitor. If mature trach, attempt replacement through stoma with confirmation. If any difficulty, convert to oral intubation.
Disposition: Fresh decannulation requires admission for observation during tract maturation, planned tracheostomy replacement when ready (typically 5-7 days later), and airway management. Mature decannulation managed with tube reinsertion; if successful replacement without difficulty, patient may be discharged if otherwise ready. Return precautions: any subsequent decannulation, difficulty breathing, stridor, or subcutaneous emphysema warrant immediate evaluation.
Tracheostomy Respiratory Distress
Patient with tracheostomy in place presents with acute respiratory distress. Patient is hypoxic, tachypneic, or using accessory muscles. First concern is tracheostomy obstruction or malfunction. Presentation may rapidly deteriorate if not rapidly managed.
Initial approach — obstruction management: Call respiratory therapy immediately. Patient assessed for ability to speak or phonation around the cuff (if present), which indicates adequate airway space. High-flow oxygen delivered by T-tube or trach mask. Attempt to pass a suction catheter through the tube — if resistance encountered, tube is obstructed. Remove the inner cannula (if present) and set aside. Attempt suction through outer cannula with large-bore suction catheter. If secretions aspirated and patient improves, replace inner cannula and reassess. If no resistance and patient remains in distress after suctioning, proceed to next step.
Cuff assessment and deflation: Assess the tracheostomy cuff pressure (should be 20-30 cm H2O). If cuff is overdistended, it may be compressing the airway distal to the tube. Cuff slowly deflated by withdrawing air from the cuff balloon — do this in small increments, listening for improvement in airflow. Ask patient if symptoms improve. If cuff malfunction suspected (air will not withdraw, or no difference noted after deflation), assume cuff failure and proceed to next step.
Tube removal and alternative airway: If obstruction persists despite inner cannula removal and suctioning, and especially if cuff dysfunction suspected, remove the entire tracheostomy tube and immediately establish alternative airway. Patient given high-flow oxygen by tight face mask or BVM. Decision tree: (1) if stoma tract mature (>7 days) and time permits, attempt to place a 6.0 cuffed ETT through the stoma over a bougie; (2) if acute distress or unable to place through stoma, proceed immediately to oral intubation via direct laryngoscopy. Once alternative airway (either stoma ETT or oral ETT) is in place, patient stabilized and diagnostic imaging obtained to determine cause of obstruction (suspected causes: mucus plug, tube malposition, granulation tissue obstruction, tracheal stenosis).
Alternative manual ventilation if intubation not immediately available: If patient in severe distress and trained provider not immediately at bedside, apply BVM directly over stoma (seal mouth with hand or tape) or use a size 2 LMA positioned over the stoma with BVM connected. This is a temporary measure — patient must be transferred for definitive airway management.
Plan: Identify and resolve obstruction. If tube malfunction or persistent obstruction despite troubleshooting, replace with new tube (through stoma if mature, or convert to oral intubation if fresh or unable to place through stoma). Obtain imaging to assess tracheal lumen and tube position. Monitor for stridor, persistent distress, or subcutaneous emphysema. If imaging reveals stenosis or granulation tissue, involve otolaryngology or interventional radiology for definitive management.
Disposition: If obstruction rapidly resolved with suctioning and inner cannula replacement, patient may be discharged after brief observation and education on cuff care and secretion management. If tube malfunction requiring replacement or concern for underlying tracheal pathology (stenosis, granulation), admit for observation, tube management, and subspecialty evaluation. Return precautions: any recurrent distress, stridor, inability to pass suction catheter, or difficulty speaking warrant immediate evaluation.
Clinical Education
Tracheostomy Anatomy and Tract Maturation
The critical distinction in tracheostomy emergency management is the maturity of the tract: fresh (7 days) tracheostomies have established epithelialized tracts and allow safe tube replacement through the stoma. [1] The 7-day threshold is not arbitrary — it reflects the time required for epithelial ingrowth to stabilize the tract walls and make blind cannulation safe.
Tract maturation timeline: During the first 48 hours post-placement, the tract is a raw wound channel with no structural support. By day 3-4, early epithelialization begins at the margins. By day 5-7, the tract is largely epithelialized but still friable and prone to bleeding or false passage if forcefully instrumented. By day 7-10, epithelialization is complete and the tract is mechanically stable. This timeline is affected by nutrition, infection, corticosteroid use, and underlying lung disease — diabetic and immunocompromised patients may require longer maturation periods.
Clinical implication: A fresh tracheostomy that is accidentally decannulated should NOT have blind replacement attempted through the stoma. The risk of false passage (tube placement into subcutaneous tissue or between muscle planes) is high, and once a false passage is created, the “stoma” is no longer usable — the patient requires oral intubation and a new tracheostomy tract when matured. Instead, secure the airway orally, stabilize the patient, and allow the tract to mature before attempting re-placement.
Stepwise Approach to Tracheostomy Emergencies
The National Tracheostomy Safety Project published a systematic algorithm for management of acute tracheostomy emergencies. [2] This algorithm guides rapid decision-making when a tracheostomy patient becomes acutely distressed or decannulated.
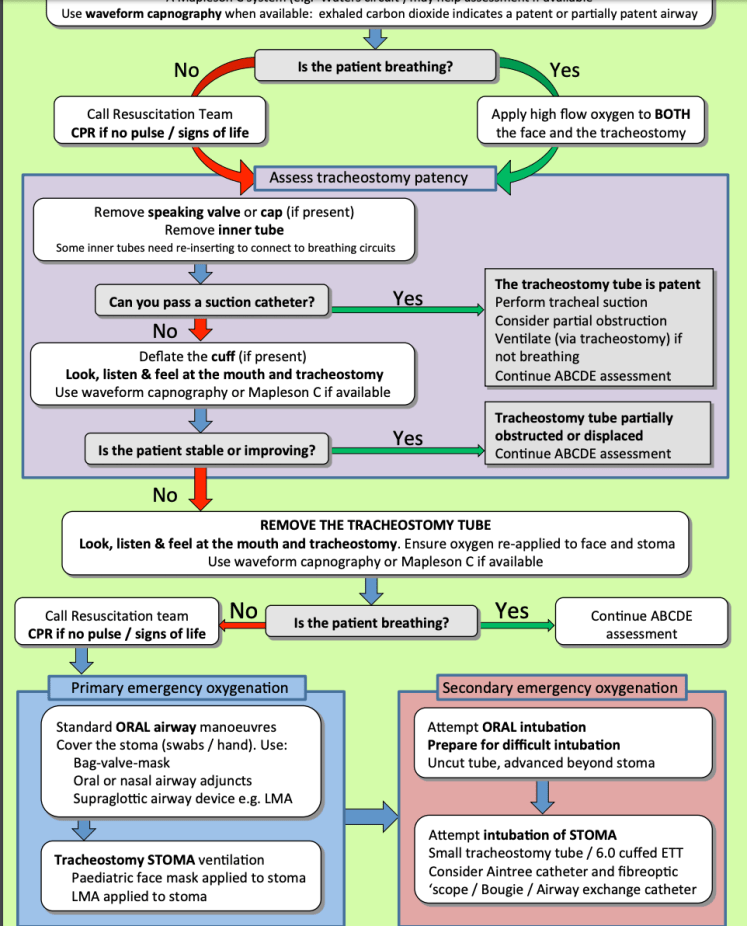
The algorithm sequence for acute distress: (1) Sit patient upright. (2) Remove inner cannula and suction aggressively. (3) Deflate the cuff. (4) If patient improves, re-inflate cuff after suction and re-insert inner cannula. If patient does not improve, (5) Remove the entire outer cannula. (6) Place a bougie through the stoma and advance a cuffed ETT over the bougie (for mature tracts only). (7) If unable to place through stoma, or if fresh tract, perform oral intubation via direct laryngoscopy. (8) Call for help, get imaging, and identify the cause of obstruction post-stabilization.
The algorithm emphasizes: do not spend time troubleshooting the original tube when the patient is in severe distress. If simple maneuvers (suctioning, cuff deflation) do not rapidly improve the patient, move to removal and alternative airway placement. The patient’s hypoxia drives the timeline.
Tracheostomy Bleeding: Superficial vs. Deep
Bleeding from a tracheostomy is common (mild bleeding occurs in up to 50% of patients in the post-operative period) but must be distinguished as superficial or deep, which carry very different implications. [3]
| Feature | Superficial Bleeding | Deep Tracheal Bleeding |
|---|---|---|
| Source | Stoma margin, cannula-tissue interface, granulation tissue | Tracheal wall, vascular erosion (innominate artery, brachiocephalic trunk) |
| Bleeding volume | Light ooze to modest volume (< 30 mL), easily controlled | Massive or rapidly increasing (may reach 100+ mL/min) |
| Response to direct pressure | Rapid control with direct pressure, silver nitrate, or hemostatic gauze | Continues despite direct pressure; may briefly slow with cuff hyperinflation |
| Hemodynamic status | Stable; no tachycardia or hypotension | Unstable or rapidly becoming unstable; tachycardia, hypotension |
| Timing | Common in first 1-2 weeks post-placement; may be recurrent with poor wound care | Usually occurs after 5+ days (vascular erosion develops over time); can be sentinel bleed before massive hemorrhage |
Superficial bleeding management: Apply direct pressure with sterile gauze for 5-10 minutes. Inspect for granulation tissue (friable red tissue at stoma margin, common cause). If bleeding continues, apply topical hemostatic agents: silver nitrate cautery (cauterize bleeding point with silver nitrate stick, brief burning sensation), thrombin-soaked gauze, or hemostatic matrix (Surgicel, FloSeal). Cuff pressure verified to be 20-30 cm H2O (excess pressure contributes to bleeding). Remove inner cannula, suction any debris, and replace. Routine wound care and gentle handling prevent recurrence.
Deep tracheal bleeding: This is a surgical emergency and likely represents vascular erosion. Do not attempt local control with direct pressure — continue suctioning and call surgery immediately. Position patient sitting upright and leaning forward (gravity assists bleeding away from airway). Keep suction at bedside. If massive bleeding with hemodynamic instability, the cuff can be hyperinflated as a temporizing measure to tamponade the bleeding vessel while emergent surgical consultation is obtained. Rigid endoscopy performed to visualize the source and guide control (possible direct vessel ligation, tracheal repair, or diversion to oral intubation with anesthesia support). Interventional radiology consulted if arterial erosion is suspected and cuff tamponade achieved.
Tracheo-Innominate Fistula: The Sentinel Bleed Concept
Tracheo-innominate fistula (TIF) is the most feared complication of tracheostomy, occurring in 0.5-1% of tracheostomy patients, with mortality exceeding 50% even with treatment. [4] The mechanism is erosion of the tracheostomy tube into the anterior tracheal wall with subsequent perforation into the innominate artery (or less commonly the brachiocephalic trunk, aortic arch, or other mediastinal vessels).
Risk factors: High cuff pressure (>30 cm H2O), low stoma placement (below the 2nd tracheal ring, closer to the innominate artery), tube movement and friction, infection, prolonged intubation, corticosteroid use (impairs healing), and diabetes. Timing is typically 5-14 days post-placement (range up to several months in chronic tracheostomy), reflecting the time required for vascular erosion to develop.
The sentinel bleed: A patient who presents with sudden brisk bleeding from a tracheostomy, especially if the bleeding arises from deep in the stoma (not the cannula-tissue margin) or continues despite direct pressure, may be experiencing the sentinel bleed of an impending TIF. This is a medical emergency. The bleeding may temporarily slow with cuff hyperinflation (external compression of the artery) but will recur. Do not wait for the massive hemorrhage before acting. Immediately call surgery, anesthesia, and interventional radiology. Prepare for emergent endoscopy, possible fistula closure, and likely transfer to the OR.
Management of suspected TIF: Once TIF is suspected, the patient is at extreme risk of exsanguinating hemorrhage. Hyperinflate the cuff immediately as a temporizing measure — this increases external pressure on the vessel and may slow bleeding enough to allow mobilization to the OR. Do not deflate the cuff without surgical backup at the bedside. Rigid endoscopy performed to confirm the diagnosis (direct visualization of pulsatile bleeding, vessel erosion, or fistula tract). Definitive treatment is surgical closure of the fistula, typically via thoracotomy with primary vessel repair or ligation (if distal brachiocephalic trunk). Some centers attempt endoscopic approaches (balloon tamponade, stent placement), but surgery remains the standard of care for confirmed TIF. Mortality is lower with early recognition and surgical intervention (50%).
Prevention: Maintain appropriate cuff pressure (20-30 cm H2O, measured weekly), ensure the stoma is placed at the appropriate level (over the 2nd tracheal ring), minimize tube movement and friction, and educate caregivers on gentle tube handling. Any recurrent or atypical bleeding warrants rigorous investigation (rigid endoscopy) rather than assumption that bleeding is benign.
Displacement Management by Tract Maturity
Accidental decannulation management is entirely determined by whether the tract is fresh or mature. [1]
Fresh tracheostomy (< 7 days): The tract is not epithelialized and is only a raw channel in loose areolar tissue. Blind re-insertion of the tube into this channel has a high risk of creating a false passage — the tube is pushed not into the trachea but into the loose tissue around the trachea, resulting in subcutaneous placement. Once a false passage is created, it becomes the “new stoma,” and the true tracheal lumen is lost. The patient’s airway is now compromised without a patent stoma. Management: Do NOT attempt blind replacement. Instead, call anesthesia stat and prepare for oral intubation. Secure the airway orally with a cuffed ETT via direct laryngoscopy. Once airway is secure, place patient on oxygen and allow the tract to mature for 7+ days before attempting re-cannulation. A new tracheostomy can be placed once the original tract has epithelialized (usually 7-10 days later) or after the oral intubation is complete, depending on clinical circumstances.
Mature tracheostomy (> 7 days): The tract is epithelialized and mechanically stable. Blind replacement through the stoma is safe. Technique: Have respiratory therapy at bedside. Place patient on high-flow oxygen by face mask. Using a bougie or small cuffed ETT (6.0 or 7.0) as a guide, gently advance the tracheostomy tube through the stoma. Once placed, inflate the cuff, secure the tube with ties or sutures, and immediately listen for bilateral breath sounds. Obtain a chest X-ray to confirm tube position (should be 2-3 cm above the carina). If any resistance encountered during placement, stop and convert to oral intubation rather than forcing the tube and risk creating a false passage. Most mature decannulations are easily resolved with simple replacement.
Special case — decannulation with stridor: If decannulation is accompanied by stridor (indicating edema or obstruction of the glottis or subglottis), do not assume the problem is the trach. The stridor may reflect post-extubation laryngeal edema or supraglottic obstruction from a prior oral intubation. Apply nebulized epinephrine and dexamethasone, and observe before attempting tracheostomy reinsertion. Once stridor resolves, proceed with trach replacement if still needed.
Respiratory Distress: Obstruction Troubleshooting
A tracheostomy patient presenting with acute dyspnea is obstructed until proven otherwise. [5] The most common causes are mucus plugging, inner cannula obstruction, cuff dysfunction, and tube malposition. The diagnostic sequence is rapid and empirical: treat what you can without delay, and only if the patient fails to improve proceed to the next intervention.
Step 1 — Suctioning: Remove the inner cannula (if present) and suction aggressively with a large-bore catheter through the outer cannula. Pass the catheter gently until resistance is met or secretions are aspirated. If abundant secretions obtained and patient improves, replace the inner cannula and reassess. Most episodes of acute distress from mucus plugging resolve with this step alone.
Step 2 — Cuff deflation: Cuff malfunction (overdistension, herniation, or rupture) can cause airway narrowing. Slowly withdraw air from the cuff balloon in small increments (5-10 mL at a time), pausing between withdrawals to assess for clinical improvement (better airflow, improved oxygen saturation, decreased work of breathing). If sudden improvement occurs after cuff deflation, cuff malfunction is the problem — the cuff will need to be replaced or the tube changed. Note: If the cuff has a leak (air does not withdraw), the problem is cuff rupture, and the tube must be replaced.
Step 3 — Tube removal and reposition: If suctioning and cuff deflation do not improve distress, remove the entire outer cannula. Provide high-flow oxygen by face mask. If the patient immediately improves, the obstruction is in the tube itself (not the airway distal to the tube) — granulation tissue, dried secretions, or tracheal stenosis has developed. Assess for ability to pass suction catheter or bougie through the stoma (confirms the stoma itself is patent). If the stoma is patent but the tube is obstructed, place a new tracheostomy tube of the same or slightly smaller size.
Step 4 — Alternative airway placement: If the patient remains in distress after tube removal, or if the stoma itself is not patent, secure an alternative airway. For mature tracheostomy, attempt to place a 6.0 cuffed ETT through the stoma over a bougie. For any patient where this fails or if acute distress, proceed to oral intubation via direct laryngoscopy. Once airway secured, obtain imaging (CXR, CT neck) to assess tracheal lumen, tube position, and presence of stenosis, granulation, or other pathology.
Equipment pearls: Standard tracheostomy tubes (Shiley metal or Portex plastic) come in sizes 6-10 mm inner diameter, with corresponding outer diameters. A size 6.0 cuffed ETT can be advanced through a mature stoma if tube replacement is needed. A bougie (gum-elastic, plastic-coated, or metal) is used to guide the tube over the stoma and prevent false passage. For immediate manual ventilation if equipment is not available, apply a BVM directly to the stoma (sealing the mouth with one hand) or use a size 2 LMA positioned over the stoma. These are temporary measures only — definitive airway management (oral intubation or new tracheostomy) must follow.
Tracheostomy Equipment and Tube Options
Shiley (metal tube) vs. Portex (plastic tube): Shiley tubes are fenestrated metal tubes with removable inner cannulas, allowing cuff deflation and assessment of airway above the stoma. They are durable and permit speaking if cuff deflated. Portex tubes are single-lumen cuffed plastic tubes, more portable but less amenable to inspection. Choice depends on patient physiology (if potential for spontaneous breathing above the stoma desired, Shiley preferred) and clinical need (if need for immediate secure airway, Portex preferred). Both are available in sizes 6-10 mm inner diameter.
Tube size selection in acute replacement: If a tracheostomy patient’s tube is obstructed or dysfunctional and replacement is needed, replace with the same size initially. If the same size cannot be placed (resistance, stricture development), use a size smaller (e.g., size 7 if original was 8). Avoid oversizing — the cuff will sit in subcutaneous space rather than in the trachea.
Guidewire and bougie placement: A flexible bougie (such as a gum-elastic or plastic-coated bougie) is passed through the stoma to ensure the plane is correct and to guide the tube over the stoma. The technique: Pass the bougie through the stoma gently until resistance is met in the trachea (usually 2-3 cm). Then thread the new tube over the bougie and advance it until seated. The bougie prevents the tube from entering a false passage or subcutaneous plane. For critical situations, a cuffed ETT (6.0) can serve as a temporary tube to be placed over the bougie and used until a formal tracheostomy tube is obtained.
Manual ventilation options: If a tracheostomy patient loses their airway and oral intubation is not immediately available, several temporary ventilation options exist: (1) BVM applied directly to the stoma (seal the mouth with tape or your hand); (2) Size 2 LMA positioned over the stoma with the cuff inflated and BVM connected; (3) Size 2.5-3 LMA used for stoma intubation if time and expertise permit. None of these is ideal for long-term ventilation, but they buy time until a definitive airway (oral intubation or new tracheostomy tube) is secured.
References
- Pandian V, Miller CR, Schiavi AJ, et al. Tracheostomy-related emergency complications: a comprehensive review. Respir Care. 2018;63(4):429-448. PubMed
- McGrath BA, Bates L, Atkinson D, Moore JA; National Tracheostomy Safety Project. Multidisciplinary tracheostomy safety guidelines. Br J Hosp Med (Lond). 2012;73(12):696-702. PubMed
- Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Richardson MA, Schuller DE, eds. Otolaryngology: Head and Neck Surgery. 4th ed. Philadelphia: Mosby; 2005.
- Kang C, Sung J, Park IS, Shim J. Tracheo-innominate artery fistula: A rare but fatal complication of tracheostomy. Korean J Crit Care Med. 2016;31(3):271-274. PubMed
- Durbin CG Jr. Techniques for performing tracheostomy. Respir Care. 2005;50(4):488-496. PubMed
