Last reviewed: March 2026
Contents
MDM Templates
Foot Fracture
Workup: XR Foot
Findings: Fracture
Consult: Podiatry/Orthopedic Surgery
Patient does not currently demonstrate complications of fracture such as compartment syndrome, arterial or nerve injury.
Interventions: The fracture has been satisfactorily immobilized, and the patient has been given appropriate analgesia.
Disposition: Discharge with strict return precautions and instructions to follow up with primary MD within 24-48 hours for further evaluation including referral to an orthopedist or podiatrist.
Ankle Sprain
Workup: XR Ankle
Findings: No fracture or dislocation.
Presentation most consistent with Ankle Sprain. Patient does not currently demonstrate complications of sprain such as compartment syndrome, arterial or nerve injury.
Disposition: Discharge. Supportive bracing provided. WBAT. RICE. Strict return precautions and instructions to follow up with primary MD within 24-48 hours for further evaluation.
Ankle Fracture
Workup: XR Ankle
Findings: Fracture
Patient does not currently demonstrate complications of fracture such as compartment syndrome, arterial or nerve injury.
Interventions: The fracture has been satisfactorily immobilized, and the patient has been given appropriate analgesia.
Consult: Podiatry or Orthopedic Surgery if Weber B with talar shift or Weber C.
Disposition: Discharge with strict return precautions and instructions to follow up with primary MD within 24-48 hours for further evaluation including referral to an orthopedist or podiatrist.
Foot Puncture Wound
Workup: XR Foot
Findings: No retained foreign body or bony fracture. No skin infectious findings.
Patient lower risk for infection given: not immunocompromised, nondiabetic, distal foot involvement.
Rx: Defer prophylactic antibiotics given low risk profile. Tetanus updated.
Disposition: Discharge. Advised patient to follow up with primary care provider for wound check in 48 hours or return to ED for worsening redness, swelling, drainage, or fever.
Higher risk (diabetic, immunocompromised, deep/proximal puncture):
Rx: Ciprofloxacin 500mg PO BID x 7 days for pseudomonal coverage with 48 hour wound follow up.
Achilles Tendon Rupture
Patient presenting with acute posterior ankle/heel pain, palpable gap in Achilles tendon, and positive Thompson test. Presentation consistent with Achilles tendon rupture.
Interventions:
- Posterior splint in gravity equinus (plantarflexion)
- Analgesia
- Strict non-weight-bearing
Consult: Orthopedic Surgery
Disposition: Discharge with orthopedic follow-up within 1 week for discussion of operative vs non-operative management.
Clinical Education
Ottawa Ankle & Foot Rules
Use the Ottawa Ankle Rule and Ottawa Foot Rule to determine need for imaging. Sensitivity approaches 100% for clinically significant fractures — the rules are designed to rule out fracture, not rule it in.[1]
Ankle XR indicated if: Bone tenderness at posterior edge or tip of either malleolus (distal 6cm), OR inability to bear weight (4 steps) immediately and in the ED.
Foot XR indicated if: Bone tenderness at base of 5th metatarsal, OR bone tenderness at the navicular, OR inability to bear weight (4 steps) immediately and in the ED.
Do NOT apply if: Age <18 (originally validated in adults, though subsequent studies support use in children ≥5), intoxicated, distracting injuries, altered mental status, or inability to cooperate with exam.[1]
Hindfoot Fractures
Calcaneus fracture: Typically from axial load (fall from height). Always check the lumbar spine — 10% have associated compression fractures. Check Bohler’s angle on lateral XR: normal = 20-40°. Flattened angle suggests depressed fracture requiring CT and ortho consult.[2]

See: Radiopaedia — Bohler’s Angle
Talar fracture: High-energy mechanism. CT generally indicated for surgical planning. Talar neck fractures risk avascular necrosis (AVN) of the talar body due to retrograde blood supply — AVN risk increases with displacement and associated dislocation. Ortho consult for all talar neck/body fractures.[3]
Subtalar dislocation: High-energy injury. Reduce with ankle in plantarflexion, then hindfoot inversion or eversion depending on direction of dislocation. Procedural sedation required. Post-reduction CT to evaluate for associated fractures.

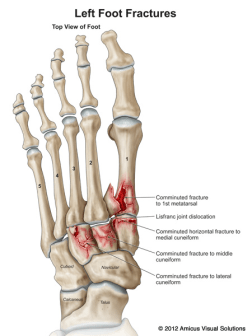
Midfoot — Lisfranc Injuries
Why it matters: The most commonly missed fracture on foot XR. Missed Lisfranc → chronic midfoot instability, arthritis, and disability. Have a low threshold to CT if clinical suspicion exists despite normal-appearing XR.[4]
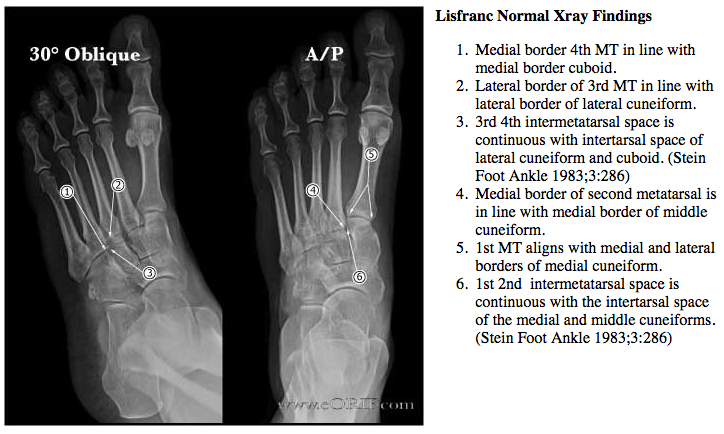
XR findings: Look for alignment of the medial border of the 2nd metatarsal with the medial border of the middle cuneiform on AP view, and medial border of the 4th metatarsal with the medial border of the cuboid on oblique view. Any step-off = abnormal. Fracture of the base of the 2nd metatarsal is pathognomonic. A “fleck sign” (small avulsion fragment between 1st and 2nd metatarsal bases) is highly suggestive.[4]
Clinical exam: Midfoot swelling and tenderness, pain with passive abduction/pronation of the forefoot, inability to bear weight. Plantar ecchymosis is a classic finding.
If unsure: CT foot, or weight-bearing XR with forefoot abduction stress views. Non-weight-bearing XR can miss subtle Lisfranc injuries.
Management: All confirmed Lisfranc injuries need ortho follow-up. Non-displaced may be managed with NWB casting; displaced injuries require ORIF. Posterior short leg splint, strict NWB, and ortho follow-up in 3-5 days from the ED.
See: Radiopaedia — Lisfranc Injury imaging
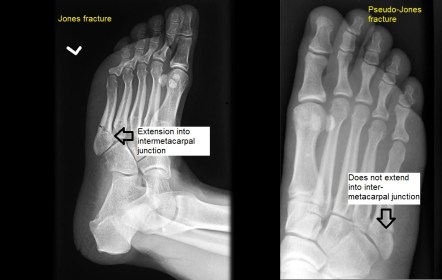
Forefoot — Jones vs Pseudo-Jones
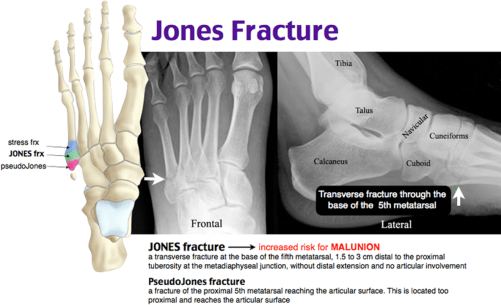
The distinction matters because management and prognosis are very different:[5]
| Pseudo-Jones (Zone 1) | Jones Fracture (Zone 2) | Stress Fracture (Zone 3) | |
| Location | Tuberosity avulsion | Meta-diaphyseal junction | Proximal diaphysis |
| Mechanism | Ankle inversion (peroneus brevis avulsion) | Acute adduction force on plantarflexed foot | Repetitive stress (runners, athletes) |
| Treatment | Walking boot, WBAT, PCP/ortho 1 week | Posterior short leg splint, strict NWB, ortho 3-5 days | Posterior short leg splint, strict NWB, ortho 3-5 days |
| Prognosis | Heals well | ~50% nonunion/re-fracture rate | High nonunion risk, often surgical |
Pseudo-Jones pearl: Ortho referral probably unnecessary unless >3mm displacement of the avulsion fragment.
Navicular fracture: Dorsal avulsion fractures are common and benign (walking boot, WBAT). Navicular body and stress fractures have high nonunion rates — NWB cast, ortho follow-up.[6]

Ankle Fracture Classification (Weber)
The Weber classification determines stability and need for operative fixation based on the level of the fibula fracture relative to the syndesmosis:[7]
| Type | Fibula fracture level | Syndesmosis | Management |
| Weber A | Below syndesmosis | Intact | Stable. Walking boot, WBAT, ortho follow-up. |
| Weber B | At syndesmosis | May be disrupted | Stability depends on talar shift. No talar shift → splint, NWB, ortho. Talar shift → ORIF. |
| Weber C | Above syndesmosis | Disrupted | Unstable. Splint, NWB, ortho consult in ED — usually ORIF. |
See: Radiopaedia — Weber Classification
Bimalleolar/trimalleolar: By definition unstable. Posterior short leg splint, strict NWB, ortho consult — these typically require ORIF.[7]
Maisonneuve fracture: Proximal fibula fracture + medial malleolus fracture or deltoid ligament tear + syndesmotic disruption. The ankle XR may only show a medial malleolus fracture or widened medial clear space — always palpate the proximal fibula and get a full-length tib/fib XR if tender. Unstable, requires ORIF.[8]
See: Radiopaedia — Maisonneuve Fracture
Achilles Rupture Pearls
Classic presentation: Sudden “pop” or sensation of being kicked in the back of the ankle during push-off activity (basketball, tennis). Palpable gap in the tendon 2-6cm above the calcaneus. Patient may still be able to plantarflex weakly (accessory muscles), so preserved plantarflexion does NOT rule out rupture.[9]
Thompson test: Patient prone, squeeze the calf — absence of passive plantarflexion = positive = rupture. Sensitivity ~96%.
Imaging: Clinical diagnosis. Ultrasound at bedside can confirm if exam equivocal — look for tendon discontinuity and hypoechoic gap. MRI generally not needed in the ED.
ED management: Posterior splint in gravity equinus (plantarflexion to approximate the torn ends), strict NWB, ortho follow-up within 1 week. Operative vs non-operative management is an outpatient decision — recent evidence (STAR trial) shows functional rehabilitation with early weight-bearing is non-inferior to surgery for most patients.[10]
Foot Puncture Pearls
Pseudomonas concern: Based on older data that Pseudomonas colonizes shoe rubber/foam. Puncture through a sneaker → Pseudomonas inoculation into deep tissue → osteomyelitis risk. This drives the ciprofloxacin recommendation in higher-risk patients.[11]
Who gets prophylactic antibiotics: No strong RCT evidence. Reasonable to give Ciprofloxacin 500mg PO BID x 7 days if: diabetic, immunocompromised, deep puncture through footwear, plantar/proximal location, delayed presentation. Low-risk punctures (clean, distal, just occurred, healthy patient) can be managed expectantly with close follow-up.
Imaging: XR to rule out retained foreign body and establish baseline. If concern for osteomyelitis on re-presentation (persistent pain/swelling at 1-2 weeks), MRI is study of choice.
Don’t forget: Tetanus status. Update Tdap if not current.
References
- Stiell IG et al. Implementation of the Ottawa Ankle Rules. JAMA. 1994;271(11):827-832. PubMed
- Mitchell MJ et al. Calcaneal Fractures. Clin Podiatr Med Surg. 2019;36(2):197-223. PubMed
- Dodd A, Lefaivre KA. Outcomes of Talar Neck Fractures: A Systematic Review and Meta-Analysis. J Orthop Trauma. 2015;29(5):210-215. PubMed
- Welck MJ et al. Clinical Characteristics of Lisfranc Injuries: A Systematic Review. Injury. 2015;46(4):734-740. PubMed
- Dean BJ et al. Fractures of the Fifth Metatarsal: Diagnosis and Management. BMJ. 2011;343:d7202. PubMed
- Defined. Navicular Stress Fractures. Clin Sports Med. 2006;25(1):53-62. PubMed
- Okanobo H et al. Simplified Classification of Ankle Fractures. Radiographics. 2012;32(3):E153-E168. PubMed
- Babbit DP. The Maisonneuve Fracture. Radiol Clin North Am. 1972;10(1):171-173. PubMed
- Maffulli N et al. Clinical Diagnosis of Achilles Tendinopathy with Tendinosis. Clin J Sport Med. 2003;13(1):11-15. PubMed
- Costa ML et al. Surgical Repair vs Rehabilitation for Acute Achilles Tendon Rupture (STAR Trial). BMJ. 2020;368:m160. PubMed
- Eidelman M et al. Plantar Puncture Wounds in Children: Analysis of 80 Hospitalized Patients. Foot Ankle Int. 2003;24(12):888-893. PubMed
