Last reviewed: March 2026Contents
MDM Templates
Hyperglycemia (No DKA)
Patient presents with hyperglycemia. They deny significant abdominal pain, nausea, vomiting, chest pain, and shortness of breath. They are well appearing, with no Kussmaul respirations, and no signs of dehydration.
History, exam, and workup reassure against dangerous consequences of hyperglycemia (DKA, HHS) and dangerous precipitants such as acute coronary syndrome, sepsis, etc.
Workup including POC glucose, BMP, and urinalysis does not demonstrate anion gap metabolic acidosis or significant ketonuria.
Plan: IVF bolus with reassessment.
If restarting metformin: Renal function and LFTs within acceptable limits for metformin use.
Disposition: Discharge with instructions to resume/adjust diabetes medications as directed. Follow up with PCP within 24-48 hours. Return precautions for vomiting, abdominal pain, confusion, or inability to keep down fluids.
Observation admission if indicated: Patient with limited access to follow-up care, poor social support, and recurrent presentations. Plan observation admission for glucose optimization and outpatient diabetes management coordination.
Insulin Pump Hyperglycemia
Patient is an insulin pump user presenting with uncontrolled hyperglycemia.
Pump was interrogated — no obvious tubing disconnection, infusion site leak, or pump malfunction identified.
Presentation not consistent with DKA or HHS. Workup does not demonstrate anion gap metabolic acidosis or significant ketonuria.
Disposition: Patient counseled on sick-day rules including increased basal rates during illness, more frequent glucose monitoring, and checking for ketones when glucose is above 250. Return precautions for persistent vomiting, abdominal pain, confusion, or glucose not responding to correction boluses.
If DKA present: Patient meets criteria for DKA. Pump disconnected at the infusion site. Transitioned to IV insulin infusion per DKA protocol. See DKA template.
DKA
Patient presents with hyperglycemia and clinical features concerning for diabetic ketoacidosis.
Workup confirms DKA:
glucose ***
pH ***,
anion gap ***
Evaluated for precipitant including infection, medication non-adherence, ACS, and other etiologies.
Plan: Aggressive IVF resuscitation with balanced crystalloids. Potassium confirmed >3.3 mEq/L prior to initiation of insulin infusion at *** U/hr. Electrolytes monitored q2h with POC glucose q1h.
Re-evaluation — improving: Glucose downtrending to ***. Anion gap narrowing to ***. Continued insulin infusion. When glucose <200, added dextrose to IV fluids and reduced insulin infusion rate by half.
Re-evaluation — DKA resolved: Anion gap closed, glucose <200, pH >7.3, bicarbonate ≥15, patient tolerating PO intake. Started basal insulin (glargine) subcutaneously at *** units. Continuing IV insulin infusion for 2 hours to overlap during transition. Prandial insulin ordered with meals.
Disposition: Admit for ongoing DKA management and insulin infusion. May transition to subcutaneous insulin once DKA resolution criteria met (anion gap <12, glucose <200, bicarb ≥15 or pH >7.3, tolerating PO).
Euglycemic DKA
Patient presents with nausea, vomiting, and malaise.
They are currently taking an SGLT2 inhibitor.
Despite glucose of only ***, workup reveals anion gap metabolic acidosis with pH ***, anion gap ***, and positive ketones — consistent with euglycemic DKA.[1]
History and exam lower suspicion for other causes of anion gap metabolic acidosis including toxic ingestion, lactic acidosis, and uremia. SGLT2 inhibitor has been held.
Plan: Treated per DKA protocol with early initiation of dextrose-containing IV fluids given near-normal glucose. Insulin infusion started at *** U/hr with potassium confirmed >3.3 mEq/L. Electrolytes and VBG monitored q2h.
Disposition: Admit for DKA management. SGLT2 inhibitor to remain held.
Clinical Education
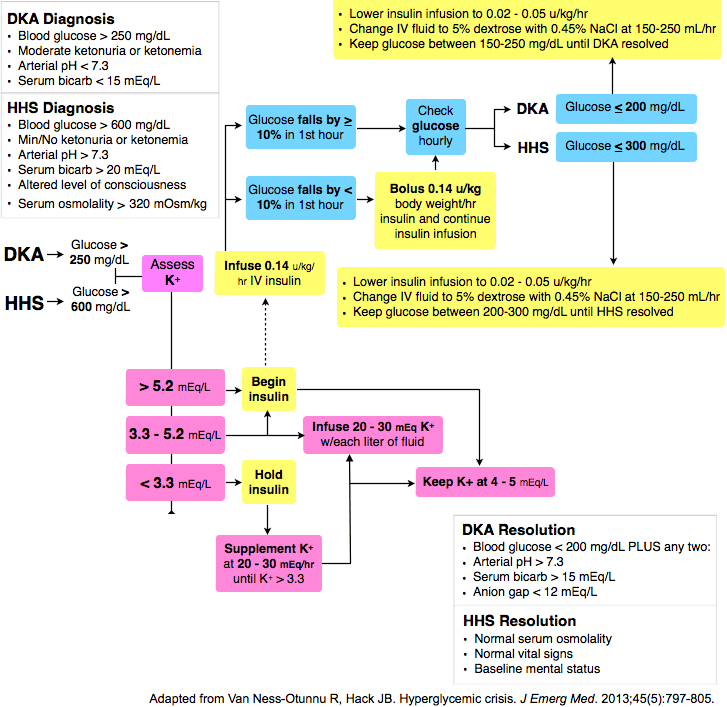
DKA vs HHS
| Feature | DKA | HHS |
| Glucose | >250 mg/dL (can be lower in euglycemic DKA) | >600 mg/dL |
| pH | <7.3 | >7.3 |
| Bicarbonate | <18 mEq/L | >18 mEq/L |
| Serum osmolality | Variable | >320 mOsm/kg |
| Ketones | Positive (serum and urine) | Absent or trace |
| Mental status | Alert to obtunded | Stupor to coma (correlates with osmolality) |
| Onset | Hours to days | Days to weeks |
| Typical patient | Type 1 (or Type 2 under stress) | Type 2 (often elderly) |
| Mortality | 1-5% | 5-20% |
Overlap exists. About 30% of patients present with features of both DKA and HHS.[2] Treat the acidosis (DKA protocol) while also addressing the profound dehydration and hyperosmolarity. These mixed presentations carry higher mortality.
DKA Treatment Protocol
Step 1 — IV Fluids: Aggressive volume resuscitation is the first priority. Start with balanced crystalloids (LR preferred over NS). NS carries risk of hyperchloremic metabolic acidosis, which can confuse anion gap trending and delay recognition of DKA resolution.[3] Typical deficit is 5-9 L. Start with 15-20 mL/kg/hr (usually 1-1.5 L) in the first hour, then reduce to 250-500 mL/hr based on hemodynamics and urine output.
Step 2 — Potassium first, then insulin. Check potassium before starting insulin. If K <3.3 mEq/L, hold insulin and replete potassium aggressively (20-40 mEq/hr IV) until K >3.3. Insulin drives potassium intracellularly and can precipitate fatal hypokalemia and arrhythmias. If K is 3.3-5.3, include 20-40 mEq KCl per liter of IV fluids. If K >5.3, hold potassium but recheck q2h.[2]
Step 3 — Insulin infusion: Start at 0.1-0.14 U/kg/hr. The initial IV bolus is no longer routinely recommended — evidence shows no benefit over starting the drip alone.[4] Flush the IV tubing with the insulin solution before connecting to the patient (insulin binds to plastic tubing). Target glucose decrease of 50-70 mg/dL per hour. If glucose does not fall by at least 50 in the first hour, double the infusion rate.
Step 4 — Dextrose bridge: When glucose drops below 200 mg/dL, add D5 to IV fluids (D5 1/2 NS at 100-200 mL/hr) and reduce insulin infusion rate by half. The goal is to keep the insulin running to close the anion gap — do not stop insulin just because glucose is normalizing.
Step 5 — Bicarbonate: Only indicated if pH <6.9. Give 100 mEq sodium bicarbonate in 400 mL sterile water with 20 mEq KCl over 2 hours. There is no evidence of benefit at pH >6.9 and it may worsen hypokalemia and paradoxical CNS acidosis.[2]
Monitoring: POC glucose every 1 hour. BMP and VBG every 2 hours. Track the anion gap — it is the best marker of DKA resolution, not glucose.
Resolution criteria: Anion gap <12 mEq/L AND glucose <200 mg/dL AND (bicarbonate ≥15 mEq/L OR venous pH >7.3) AND patient tolerating oral intake.
Euglycemic DKA Pearls
SGLT2 inhibitors are the primary culprit. Empagliflozin, dapagliflozin, canagliflozin, and ertugliflozin cause glycosuria, which lowers serum glucose while ketogenesis continues unchecked. Patients present with DKA but glucose may be <250 or even normal.[1]
The diagnostic trap: Because glucose is not strikingly elevated, these patients are frequently missed. Any patient on an SGLT2 inhibitor presenting with nausea, vomiting, malaise, or dyspnea should have a VBG and ketones checked regardless of glucose level. An unexplained anion gap metabolic acidosis in a patient on an SGLT2i is euglycemic DKA until proven otherwise.
Other causes of euglycemic DKA include pregnancy, starvation, heavy alcohol use, and chronic liver disease. It can also occur in type 1 diabetics who have been partially treated with insulin or who have been restricting carbohydrates.
Treatment is the same as DKA with one key difference: start dextrose-containing IV fluids early (often from the outset) since glucose is already near-normal. Target glucose 150-200 mg/dL to allow continued insulin infusion to close the gap. Hold the SGLT2 inhibitor and coordinate with endocrinology and PCP for medication reconciliation at discharge.[5]
HHS Management
HHS kills with dehydration, not acidosis. Mortality is 5-20% — much higher than DKA — and is driven by profound volume depletion (average deficit 8-12 L), hyperosmolarity, and the comorbidities of the typically elderly patient population.[6]
Fluids are the priority. Start with isotonic crystalloid (LR or NS) at 15-20 mL/kg/hr for the first 1-2 hours. Once hemodynamically stable, switch to 0.45% NS at 250-500 mL/hr if corrected sodium is elevated. Replace roughly half the fluid deficit in the first 12 hours. Overly rapid correction of osmolality risks cerebral edema — target osmolality decrease of 3-8 mOsm/kg/hr.
Insulin is secondary and lower-dose. Many protocols recommend starting with fluids alone for the first 1-2 hours. When insulin is started, use a lower rate than DKA protocols — 0.02-0.05 U/kg/hr initially. Glucose will often drop significantly with fluids alone. Target glucose decrease of 50-75 mg/dL per hour (too-rapid correction of glucose shifts water into cells and can worsen cerebral edema).[2]
Watch for: Underlying precipitant (most commonly infection — UTI and pneumonia are frequent), DVT/PE from hyperviscosity, rhabdomyolysis, and acute kidney injury. These patients need ICU-level monitoring.
Insulin Transition: IV to SC
When to transition: DKA resolution criteria met (AG <12, glucose <200, bicarb ≥15 or pH >7.3) AND patient tolerating oral intake.
Calculating the total daily dose (TDD): Take the average hourly insulin infusion rate over the last 6-8 stable hours, multiply by 24, then multiply by 0.7-0.8 to account for the difference in bioavailability between IV and SC insulin.[7]
| Step | Details |
| 1. Calculate TDD | Average hourly rate × 24 × 0.7 |
| 2. Basal insulin | 50% of TDD as glargine (Lantus) once daily |
| 3. Prandial insulin | Remaining 50% divided by 3 meals as rapid-acting (lispro/aspart) before each meal |
| 4. Overlap | Continue IV insulin for 2 hours after first SC basal dose (glargine takes 2-4 hours for onset) |
| 5. Correction scale | Add sliding scale with meals. If 2 consecutive BG readings >250, consider returning to IV insulin |
If discharging after mild DKA: Total daily basal insulin can be estimated at approximately 80% of the 24-hour IV requirement. Ensure patient has insulin, supplies, and follow-up within 24-48 hours before discharge.
New-onset diabetes without prior insulin use: Start weight-based dosing at 0.3-0.5 U/kg/day. Give 50% as basal (glargine) and 50% split across 3 meals as rapid-acting (lispro or aspart). Err on the lower end and titrate up — hypoglycemia in a discharged patient is more dangerous than a few days of mild hyperglycemia.
Airway Management in DKA
Avoid intubation if at all possible. Patients in DKA compensate for their metabolic acidosis with Kussmaul respirations — respiratory rates of 30-40+ with large tidal volumes. This compensatory minute ventilation is extremely difficult to replicate on a ventilator, and if you fail to match it, the resulting acute rise in PaCO2 will worsen acidosis and can precipitate cardiac arrest.[8]
If intubation is unavoidable (true obtundation, airway not protected): pre-oxygenate aggressively with BVM-assisted ventilations to maintain minute ventilation during the apneic period. Use ketamine for induction (hemodynamically neutral, does not suppress respiratory drive as quickly). Immediately post-intubation, set the ventilator to match their pre-intubation respiratory rate and tidal volume. A reasonable starting point is RR 30, TV 500-600 mL. Check a VBG within 15 minutes of intubation to verify adequate ventilation.
Push bicarb during RSI? Some experts advocate giving 1-2 amps of sodium bicarbonate IV push during the peri-intubation period to buffer the expected rise in CO2 during the apneic window. This is not standard protocol but is a reasonable consideration in patients with pH <7.1.
Precipitant Workup
Always search for a trigger. DKA and HHS rarely occur in isolation — identifying and treating the precipitant is as important as managing the hyperglycemic crisis itself.[2]
| Precipitant | Notes |
| Infection | Most common precipitant (30-50%). UTI and pneumonia lead. Get UA, CXR, blood cultures. Note: WBC is often elevated from stress demargination in DKA even without infection. |
| Insulin non-adherence | Most common in young type 1 diabetics. Ask about cost, access, and psychosocial barriers. Pump malfunction in pump users. |
| Infarction | ACS can precipitate DKA and may present atypically (abdominal pain, vomiting). Get an ECG and troponin on every DKA patient. |
| Intoxication | Alcohol, cocaine, and sympathomimetics. Check tox screen if history is suggestive. |
| Iatrogenic | Corticosteroids, SGLT2 inhibitors (euglycemic DKA), atypical antipsychotics, thiazides, and immunotherapy (checkpoint inhibitors causing autoimmune diabetes). |
| Initial presentation | New-onset type 1 diabetes. DKA may be the first presentation, especially in children and young adults. Check A1c. |
Standard precipitant workup: CBC, BMP, magnesium, phosphorus, troponin, ECG, UA with culture, blood cultures, CXR, lipase if abdominal pain is prominent, and beta-hCG in women of reproductive age.
Starting Insulin from the ED
This is one of the most undertaught skills in EM. Most ED docs are comfortable running an insulin drip for DKA but freeze when it comes to sending a patient home on a new insulin regimen. The approach is simpler than it seems — and the RABBIT 2 trial showed that basal-bolus insulin is superior to sliding scale alone for glycemic control, even in the inpatient setting.[9] The same principle applies at discharge: give a structured basal ± prandial regimen, not just a sliding scale.
The simple approach for the ED:
| Step | What to do |
| 1. Pick a total daily dose | 0.3-0.5 U/kg/day. Start at the low end (0.3 U/kg) — hypoglycemia at home is more dangerous than a few days of glucose in the 200s. For elderly, renal impairment, or low BMI: start at 0.2 U/kg/day.[10] |
| 2. Basal only vs basal-bolus | Most ED discharges = basal only. Give the full calculated dose as once-daily glargine (Lantus) or detemir (Levemir). Adding prandial insulin increases complexity and hypoglycemia risk — save it for endocrine follow-up. Basal-only initiation is endorsed by ADA as a safe starting strategy.[11] |
| 3. Prescribe the right things | Insulin pen or vial + syringes, pen needles, glucometer + test strips, lancets. Insulin pens are strongly preferred — they reduce dosing errors and are easier for insulin-naive patients.[12] |
| 4. Teach 3 things | (1) How to inject (abdomen, rotate sites). (2) Signs of low blood sugar (shaking, sweating, confusion) and what to do (eat 15g fast carbs, recheck in 15 min). (3) When to come back (vomiting, unable to eat, glucose >500, confusion). |
| 5. Close the loop | PCP or endocrine follow-up within 1 week (ideally 48-72 hours). The outpatient team will titrate up, add prandial insulin if needed, and optimize the regimen. Your job is to get them started safely. |
Example discharge Rx for a 80 kg patient: TDD = 0.3 × 80 = 24 units. Prescribe glargine (Lantus) 24 units SC once daily at bedtime. Prescribe insulin pen + pen needles, glucometer kit with test strips and lancets. Instruct to check fasting glucose each morning. Follow up with PCP in 48-72 hours for titration.
What about cost? Insulin cost is a major barrier. NPH insulin (available over the counter at some pharmacies as ReliOn brand for ~$25/vial) is a reasonable alternative if the patient cannot afford glargine. Dose NPH at 0.2 U/kg BID (morning and bedtime). The tradeoff is a less predictable pharmacokinetic profile and higher hypoglycemia risk, but it is far better than no insulin. Walmart and some state programs offer low-cost insulin options.[13]
Post-DKA discharge insulin: If transitioning a patient who was on an insulin drip, calculate TDD as described in the insulin transition section above (average hourly rate × 24 × 0.7). Give 50% as basal. Only discharge if DKA has fully resolved, patient is tolerating PO, and close follow-up is confirmed. The ADA recommends against discharge on the same calendar day as DKA resolution.[11]
References
- Peters AL, Buschur EO, Buse JB, et al. Euglycemic diabetic ketoacidosis: a potential complication of treatment with sodium-glucose cotransporter 2 inhibition. Diabetes Care. 2015;38(9):1687-1693. PubMed
- Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335-1343. PubMed
- Self WH, Evans CS, Jenkins CA, et al. Clinical effects of balanced crystalloids vs saline in adults with diabetic ketoacidosis: a subgroup analysis of cluster randomized clinical trials. JAMA Netw Open. 2020;3(11):e2024596. PubMed
- Gosmanov AR, Gosmanova EO, Kitabchi AE. Hyperglycemic crises: diabetic ketoacidosis and hyperglycemic hyperosmolar state. In: Endotext. MDText.com; Updated May 2021. NCBI Bookshelf
- Goldenberg RM, Berard LD, et al. SGLT2 inhibitor-associated diabetic ketoacidosis: clinical review and recommendations for prevention and diagnosis. Clin Ther. 2016;38(12):2654-2664. PubMed
- Pasquel FJ, Umpierrez GE. Hyperosmolar hyperglycemic state: a historic review of the last decade. Diabetes Care. 2014;37(11):3124-3131. PubMed
- Umpierrez GE, Hellman R, Korytkowski MT, et al. Management of hyperglycemia in hospitalized patients in non-critical care setting: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97(1):16-38. PubMed
- Long B, Koyfman A. Emergency medicine myths: diabetic ketoacidosis. J Emerg Med. 2017;53(4):590-598. PubMed
- Umpierrez GE, Smiley D, Zisman A, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 trial). Diabetes Care. 2007;30(9):2181-2186. PubMed
- American Diabetes Association. Standards of Care in Diabetes — 2024. Sec. 9: Pharmacologic approaches to glycemic treatment. Diabetes Care. 2024;47(Suppl 1):S158-S178. ADA
- American Diabetes Association. Standards of Care in Diabetes — 2024. Sec. 16: Diabetes care in the hospital. Diabetes Care. 2024;47(Suppl 1):S295-S306. ADA
- Guo RX, Zhang Y, et al. Insulin pen devices versus syringes: meta-analysis of adherence, glycemic control, and hypoglycemia. J Diabetes Sci Technol. 2021;15(3):586-595. PubMed
- Cefalu WT, Dawes DE, Gavlak G, et al. Insulin access and affordability working group: conclusions and recommendations. Diabetes Care. 2018;41(6):1299-1311. PubMed
