Last reviewed: March 2026
Contents
MDM Templates
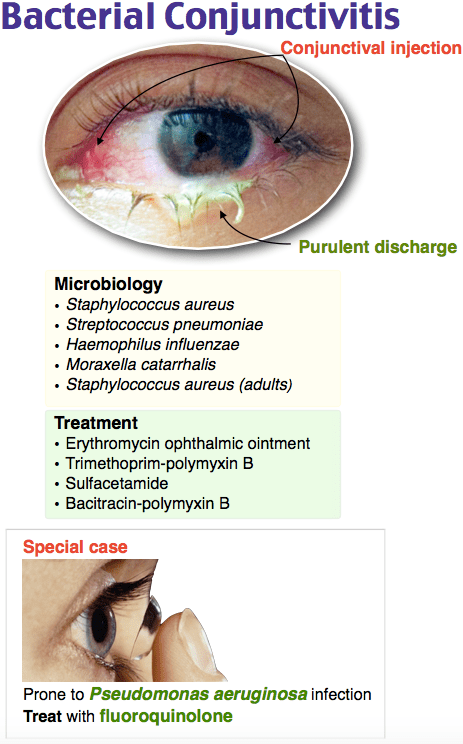
Conjunctivitis
Patient presents with red eye, discharge, and conjunctival injection. No recent eye trauma or suspected foreign body. No significant photophobia. No vision loss. Negative Seidel sign. IOP normal.
History and exam reassure against corneal abrasion or ulcer, globe rupture, uveitis, HSV keratitis, endophthalmitis, retinal detachment, acute angle-closure glaucoma, and foreign body. Well appearing without orbital signs.
Plan: Polymyxin B/trimethoprim (Polytrim) 2 drops every 6 hours for 7 days. Artificial tears 4–6 times daily for comfort.
Contact lens wearer: Fluoroquinolone drops (levofloxacin 0.5% or moxifloxacin 0.5%) to cover Pseudomonas. Strict contact lens holiday until cleared by ophthalmology.
Allergic conjunctivitis: Antihistamine drops (ketotifen 1 drop every 8 hours) and cool compresses.
Disposition: Discharge with PCP or ophthalmology follow-up if not resolving within 5–7 days.
Subconjunctival Hemorrhage
Patient presents with painless unilateral red eye consistent with subconjunctival hemorrhage. No vision changes, no trauma, no pain, no photophobia. Slit lamp exam confirms blood beneath the conjunctiva without deeper involvement.
History and exam reassure against globe rupture, hyphema, uveitis, and other dangerous causes of red eye. No signs of bleeding diathesis or coagulopathy.
Plan: No treatment required — resolves spontaneously over 1–2 weeks. Artificial tears for comfort if desired.
Recurrent episodes or spontaneous bilateral: check blood pressure, PT/INR if on anticoagulation, and consider bleeding workup.
Disposition: Discharge. No follow-up needed unless recurrent.
Corneal Abrasion
Patient presents with eye pain, tearing, and foreign body sensation after ***. Slit lamp with fluorescein demonstrates corneal epithelial defect. No Seidel sign (ruling out full-thickness injury). No infiltrate or hypopyon to suggest ulceration or infection. No foreign body retained.
History and exam reassure against globe rupture, corneal ulcer, uveitis, and retained foreign body. Visual acuity preserved or minimally reduced from baseline.
Plan: Erythromycin ointment applied, prescribed erythromycin ointment QID for 5 days. Artificial tears for comfort.
Contact lens wearer: Fluoroquinolone drops instead of erythromycin. No patching. Contact lens holiday until healed and cleared by ophthalmology.
Disposition: Discharge with ophthalmology follow-up in 24–48 hours if large abrasion or not improving. Return precautions for worsening pain, vision loss, or purulent discharge.
Corneal Foreign Body
Patient presents with eye pain and foreign body sensation after ***. Slit lamp identifies a superficial foreign body on the corneal surface. No Seidel sign. No evidence of penetrating injury. EOM intact.
History and exam reassure against globe rupture and intraocular foreign body. No deep stromal involvement.
Plan: Foreign body removed under slit lamp with needle tip / eye spud after topical anesthesia. Rust ring addressed with burr if present. Erythromycin ointment QID for 5 days.
Disposition: Discharge with ophthalmology follow-up in 24–48 hours. Return precautions for worsening pain, vision changes, or discharge.
Clinical Education
Approach to the Red Eye
Five questions that sort benign from dangerous: (1) Is there vision loss? (2) Is there significant pain (not just irritation)? (3) Is there photophobia? (4) Is the pupil abnormal? (5) Is IOP elevated? A “yes” to any of these demands slit lamp exam and consideration of serious pathology (glaucoma, uveitis, keratitis, endophthalmitis).[1]
Pattern of injection matters: diffuse conjunctival injection (pink) suggests conjunctivitis. Ciliary flush (perilimbal ring of deep injection) suggests iritis, keratitis, or glaucoma. Sectoral injection with a visible blood patch is subconjunctival hemorrhage.[1]
Conjunctivitis Pearls
Most conjunctivitis is viral and self-limited (1–2 weeks). Even culture-proven bacterial conjunctivitis often resolves without antibiotics. However, antibiotic drops speed recovery, reduce transmissibility, and allow earlier return to work/school. Prescribing antibiotics for presumed bacterial conjunctivitis is reasonable standard practice.[2]
If unresponsive to antibiotics for 1 week, consider chlamydial or gonococcal conjunctivitis. Gonococcal conjunctivitis presents with copious purulent discharge and is an ophthalmologic emergency — can perforate the cornea. Treatment: ceftriaxone 1 g IM. Chlamydial: azithromycin 1 g PO single dose.[2]
Contact Lens Wearer Red Flags
Contact lens wearers with a red eye need fluoroquinolone coverage for Pseudomonas. Never prescribe aminoglycoside or polymyxin-based drops alone in a contact lens wearer — Pseudomonas keratitis is the primary concern and can rapidly destroy the cornea. Strict contact lens holiday until cleared by ophthalmology. Overwear with extended-wear lenses is the most common risk factor.[3]
HSV Keratitis
Dendritic ulcer on fluorescein staining is pathognomonic for HSV keratitis. Look for a branching, tree-like pattern with terminal bulbs under cobalt blue light. History of prior herpes labialis or recurrent unilateral red eye increases suspicion. Treatment: oral valacyclovir 500 mg TID for 7–10 days (or topical ganciclovir gel). Do NOT prescribe topical steroids — steroids worsen HSV keratitis and can cause corneal melting. Urgent ophthalmology referral.[4]
Corneal Abrasion Pearls
Do not patch corneal abrasions. Patching does not improve healing, increases infection risk, and impairs the patient’s functional vision. Topical NSAIDs (ketorolac 0.5% QID) provide good pain relief as an adjunct to oral analgesics. Cycloplegics (cyclopentolate 1%) can reduce ciliary spasm pain in large abrasions but are not routinely needed.[5]
Contact lens–related abrasions get fluoroquinolone drops, not erythromycin — same Pseudomonas logic as above. Never prescribe topical anesthetics for home use (delays healing, risk of corneal melting).
Slit Lamp Essentials
Seidel test: apply fluorescein, look for streaming (bright green rivulet) from a wound site under cobalt blue light — positive Seidel sign means full-thickness corneal or scleral wound (globe rupture). Stop the exam, place a rigid eye shield, and call ophthalmology emergently.[1]
Cells and flare in the anterior chamber indicate iritis/uveitis. Cells are white blood cells floating in the aqueous humor (sparkling dots in the slit beam). Flare is protein leakage giving the beam a foggy appearance. Consensual photophobia (pain in the affected eye when light is shone in the opposite eye) is a bedside clue to iritis even without a slit lamp.
Disposition
Simple conjunctivitis, subconjunctival hemorrhage, small corneal abrasion: discharge with PCP follow-up. Contact lens–related keratitis, corneal ulcer, or any corneal infiltrate: same-day ophthalmology. Suspected HSV keratitis, hypopyon, globe rupture, or acute vision loss: emergent ophthalmology consultation.[1]
References
- Leibowitz HM. The Red Eye. N Engl J Med. 2000;343(5):345-351. PubMed
- Azari AA, Barney NP. Conjunctivitis: a systematic review of diagnosis and treatment. JAMA. 2013;310(16):1721-1729. PubMed
- Stapleton F et al. Risk factors for contact lens–related microbial keratitis. Ophthalmology. 2008;115(10):1655-1662. PubMed
- White ML, Chodosh J. Herpes simplex virus keratitis: a treatment guideline. AAO Preferred Practice Pattern. 2023.
- Turner A, Rabiu M. Patching for corneal abrasion. Cochrane Database Syst Rev. 2006;(2):CD004764. PubMed
