Mild Fever/Viral/improved in ED (no labs)
Patient well appearing, nontoxic.
Given history and exam, low suspicion for serious bacterial infection including but not limited to meningitis, pneumonia, UTI or bacteremia.
Likely viral etiology.
Discussed low risk but possible UTI and offered urine sampling, but mutual decision to defer urine testing as asymptomatic to best of parents knowledge.
Reassessment
Tolerating PO and appearing euvolemic. Mild fever and well appearing after antipyretic/analgesic administration.
Patient now consolable and well appearing in ED. Discussed alternating tylenol and ibuprofen as directed over the counter for antipyresis.
Disposition
Discussed strict return precautions for worsening of symptoms, increased respiratory effort, signs of CNS infection including but not limited to changes in mental status or vomiting, or fever for more than 5 days. Discussed prompt follow up with pediatrician in 24-48 hours for recheck or return to ED sooner if concerned or if cannot schedule appointment.
Discharge home
Fussy Infant MDM
No evidence of strep pharyngitis at this time.
No evidence of torsion.
Patient without diarrhea or concerning pulmonary exam findings.
Given history and exam, no overt evidence of emergent intra-abdominal process, corneal abrasion or tourniquets causing fussiness
Plan discharge home.
- Colic
- Possible colic; discussed use of soothing activities, feeding more frequently, use of pacifier.
- Definition of colic: Crying for ≥3hr/day for ≥3 days/week per week over a 3-week period in an infant <4months old.
PEARLS
- Febrile Infant
- Decision Rules for admission vs. outpatient management.
- Rochester, Philadelphia and Boston Criteria
- Caveats: Made in 90s before HiB and pneumococcal vaccines in children, maternal GBS screening
- Rochester, Philadelphia and Boston Criteria
- For any patient: Treat the cause of the fever. There is no evidence that reducing a fever decreases the morbidity or mortality of an illness, with the possible exception of patients who are critically ill or cannot tolerate the metabolic demands of a fever.
- “This includes patients with an already elevated metabolic state (shock, burns, and post-operative patients), patients with major head trauma, post-cardiac arrest, or those with underlying neurologic or cardiopulmonary disease such as cardiomyopathy” Rosh Review
- External cooling: maybe to make the child feel better, otherwise for heat stroke
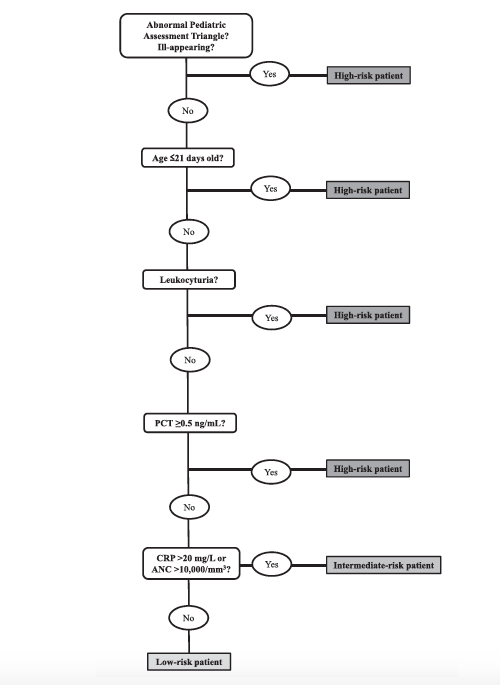
- “Step-by-Step” approach a study…
- looking at patients without lumbar puncture or empiric antibiotic treatment?
- Population
- Infants 90 days old or younger
- “fever without a source”
- Including: No pulmonary exam findings, No diarrhea.
- Workup:
- Blood culture, Urine Culture, Urine dipstick, PCT, CRP or WBC
- Algorithm
- Decision Rules for admission vs. outpatient management.
- Positive UTI <60 days old: admit for antibiotics, observation and possible renal imaging inpatient
- Generally oral ABX are not well absorbed through the gut at this age especially while sick, cephalosporins have been specifically studied.
- Admit for 3 days of IV ABX and allow patient to finish out on orals at home
- Generally oral ABX are not well absorbed through the gut at this age especially while sick, cephalosporins have been specifically studied.

- If neonatal, do the whole work up and treat for presumed meningitis until proven otherwise with amp + gent
- Don’t delay ABX for CSF
- If neonatal, do the whole work up and treat for presumed meningitis until proven otherwise with amp + gent