Last reviewed: March 2026
Contents
MDM Templates
Suicidal Ideation
Patient presents with suicidal ideation. Thought process is linear and organized. Denies auditory hallucinations, visual hallucinations, and homicidal ideation. History of prior suicide attempt by *** and prior psychiatric hospitalizations.
No overt toxidrome on exam. Well appearing with stable vitals. Presentation not consistent with toxic ingestion, anemia, hypothyroidism, infection, or intracranial pathology as the driver of psychiatric symptoms.[1]
Plan: Psychiatry consulted to evaluate for danger to self and need for involuntary hold. Admit to psychiatry for further management.
Suicidal Ideation — Discharge
Patient evaluated by both emergency medicine and psychiatric professionals and deemed safe for discharge at this time. Patient denies current suicidal ideation, has no active plan or intent, and has identified protective factors. They have a plan for psychiatric follow-up and a safe living situation with access to support.
Risk assessment considered static factors (prior attempts, psychiatric history, substance use) and dynamic factors (current ideation, plan, intent, access to means, social support). Current risk assessment supports safe discharge with outpatient follow-up.[1]
Plan: Safety plan reviewed with patient including warning signs, coping strategies, reasons for living, and emergency contacts. Lethal means counseling provided. Outpatient psychiatric follow-up arranged. Return for recurrence of suicidal thoughts, worsening symptoms, or any safety concerns.
Acute Agitation
Patient presents with acute agitation requiring emergent management for safety of patient and staff. Unable to obtain reliable history given current behavioral state.
Differential for acute agitation includes primary psychiatric disorder (psychosis, mania, personality disorder), substance intoxication or withdrawal, delirium from medical cause (infection, metabolic derangement, intracranial pathology), and pain. Must rule out medical causes before attributing agitation to psychiatric etiology alone. No overt toxidrome identified on available exam.[2]
Plan: Chemical sedation for safety. Psychiatry consulted after medical workup and once patient is able to participate in evaluation. Disposition based on underlying etiology and psychiatric assessment.
If calms with intervention: Patient responded to medication and de-escalation. Both teams agree patient is no longer a danger to self or others. Discharge with outpatient follow-up if appropriate.
Gravely Disabled
Patient presents with disorganized thought process, discordant mood and affect, and inability to care for self. Avoids conversation. No suicidal or homicidal ideation expressed. No history of prior suicide attempt.
Decision-making capacity is impaired. Patient is unable to perform activities of daily living and is without appropriate caregivers to assist. Not consistent with toxic ingestion, anemia, hypothyroidism, infection, or intracranial pathology based on history and exam.[1]
Plan: Psychiatry consulted to evaluate for grave disability and need for involuntary hold. Admit to psychiatry for further management and stabilization.
Clinical Education
Suicide Risk Assessment
No validated tool reliably predicts individual suicide risk. The Columbia Suicide Severity Rating Scale (C-SSRS) is widely used to standardize screening but should not replace clinical judgment. Risk assessment is a clinical synthesis, not a checklist score.[1]
High-risk static factors: prior suicide attempt (strongest predictor), psychiatric diagnosis (depression, bipolar, schizophrenia, borderline personality disorder), substance use disorder, male sex, older age, chronic pain, family history of suicide.
High-risk dynamic factors (modifiable, assess in real-time): current plan with intent, access to lethal means (especially firearms), recent loss or stressor, hopelessness, social isolation, recent discharge from psychiatric facility, intoxication.
Lethal means counseling is one of the most effective ED interventions. Asking about and counseling on access to firearms and medications reduces suicide completion. Provide safe storage resources for firearms and recommend locking up medications.
Agitation Management
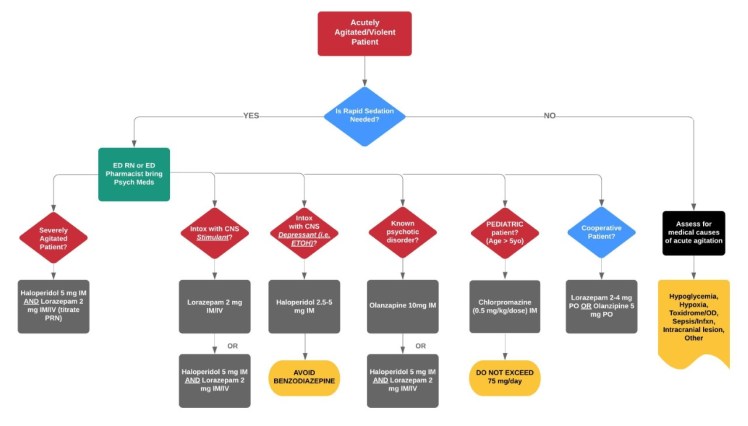
De-escalation first. Verbal de-escalation succeeds in the majority of agitated patients and should be attempted before chemical sedation unless the patient poses an immediate physical threat. Approach calmly, maintain safe distance, acknowledge the patient’s distress, offer choices.[2]
Chemical sedation when needed:
| Regimen | Dose | Notes |
| Haloperidol + lorazepam + diphenhydramine (“B52”) | 5 mg / 2 mg / 50 mg IM | Classic IM cocktail, reliable sedation |
| Olanzapine IM | 10 mg IM | Do NOT combine with IM benzodiazepines (respiratory depression risk) |
| Ketamine | 4 mg/kg IM | Fastest onset, most reliable. Prepare for airway management |
| Midazolam IM | 5 mg IM | Fastest onset benzodiazepine IM |
Do not combine IM olanzapine with IM benzodiazepines. This combination carries risk of significant respiratory depression and hypotension. If a benzodiazepine is needed after olanzapine, wait and monitor closely.
Pediatric agitation: Haloperidol or olanzapine preferred over chlorpromazine (higher sedation and dystonic effects in children). Dose-reduce appropriately.
Medical Clearance
“Medical clearance” is a misnomer — the goal is identifying medical causes of psychiatric symptoms. A focused history, physical exam, and point-of-care glucose are sufficient for the majority of psychiatric patients without medical complaints. Routine lab panels and imaging in otherwise healthy, young psychiatric patients have very low yield.[3]
When to broaden the medical workup: new-onset psychiatric symptoms without prior history, age >40 with first psychotic episode, altered mental status beyond expected psychiatric presentation, abnormal vital signs, focal neurologic deficits, history of recent substance use or overdose, medical comorbidities, or symptoms not consistent with known psychiatric diagnosis.
Acetaminophen and salicylate levels should be obtained in any patient presenting after intentional ingestion or overdose attempt, regardless of stated substances. These are the two most commonly available and dangerous OTC medications.
Involuntary Holds
Criteria for involuntary psychiatric hold (varies by state but generally requires one or more): danger to self, danger to others, or gravely disabled (unable to provide for basic needs of food, shelter, and clothing due to mental illness).
The emergency physician can initiate an involuntary hold when psychiatric consultation is not immediately available. This is a temporary measure to ensure patient safety while awaiting definitive psychiatric evaluation. Document the specific behaviors and statements that support the hold criteria.
Patients on involuntary holds still have rights including the right to be informed of the hold, the right to legal representation, and the right to a hearing. Holds have specific time limits that vary by jurisdiction.
Decision-Making Capacity
Capacity is decision-specific, not global. A patient may lack capacity for one decision (refusing life-saving treatment) while retaining capacity for another (choosing what to eat). Psychiatric diagnosis alone does not eliminate capacity.[3]
Four elements of capacity: (1) Understanding — patient comprehends the information provided about their condition and treatment. (2) Appreciation — patient recognizes how the information applies to their situation. (3) Reasoning — patient can weigh risks and benefits and explain their rationale. (4) Expressing a choice — patient can clearly communicate a consistent decision.
Document the capacity assessment. Record the specific questions asked and the patient’s responses. If capacity is questionable, psychiatry consultation is appropriate but not always required — any physician can assess capacity.
Disposition
Admit (psychiatry): Active suicidal ideation with plan or intent. Recent serious suicide attempt. Psychosis with inability to care for self. Grave disability. Involuntary hold criteria met. Homicidal ideation with identifiable target.
Discharge: Passive suicidal ideation without plan, intent, or access to means, with identified protective factors and outpatient follow-up. Agitation that resolves with treatment and patient is at baseline. Evaluated by both ED and psychiatry and deemed safe. Safety plan completed. Lethal means counseling documented. Return for worsening thoughts, inability to stay safe, or any emergency.
References
- Betz ME, Boudreaux ED. Managing suicidal patients in the emergency department. Ann Emerg Med. 2016;67(2):276-282. PubMed
- Wilson MP, Pepper D, Currier GW, et al. The psychopharmacology of agitation: consensus statement of the AAEP project BETA psychopharmacology workgroup. West J Emerg Med. 2012;13(1):26-34. PubMed
- Nazarian DJ, Broder JS, Thiessen ME, et al. Clinical policy: critical issues in the diagnosis and management of the adult psychiatric patient in the emergency department. Ann Emerg Med. 2017;69(4):480-498. PubMed
