Last reviewed: March 2026Contents
MDM Templates
STEMI — Cath Lab Activation
Patient presents with acute chest pain and ECG demonstrating ST-segment elevation consistent with acute myocardial infarction. Patient received *** in the field.
History and exam lower suspicion for aortic dissection, pericarditis/tamponade, and tension pneumothorax as alternative causes of ST elevation. No pulse differential, no tearing quality to pain, no pericardial friction rub.
Bedside ultrasound demonstrates no tamponade effusion or D sign.
Interventions:
Antiplatelet: ASA 325 mg PO. P2Y12 inhibitor: *** (ticagrelor 180 mg PO / clopidogrel 600 mg PO) per cardiology recommendation.
Anticoagulation: Heparin *** (unfractionated heparin bolus 60 U/kg [max 4,000 U] followed by 12 U/kg/hr [max 1,000 U/hr]).
Additional: IV access x2, fentanyl *** mcg IV for ischemic pain, ondansetron 4 mg IV PRN nausea. No supplemental oxygen — patient is not hypoxic.
Cardiology consulted and Cath lab activated.
Disposition: Admit directly to cardiac catheterization laboratory for emergent PCI.
STEMI Equivalent / Occlusion MI
Patient presents with *** (chest pain / dyspnea / diaphoresis) and
ECG findings consistent with a STEMI equivalent pattern —***
(posterior MI: ST depression V1–V3 with tall R waves and upright T waves /
de Winter T waves: upsloping ST depression with symmetric T-wave peaking in precordial leads /
Wellens syndrome: deeply inverted or biphasic T waves V2–V3 in pain-free interval /
new LBBB with positive modified Sgarbossa criteria /
aVR elevation with diffuse ST depression).
History and exam lower suspicion for aortic dissection, pericarditis, and tension pneumothorax as alternative causes of ECG abnormalities. Clinical picture is most consistent with acute coronary occlusion despite the absence of classic STEMI criteria on standard 12-lead ECG.
Cardiology consulted — cath lab activation for suspected occlusion MI.
Disposition: Admit directly to cardiac catheterization laboratory.
Fibrinolytic Therapy
Patient presents with ECG evidence of STEMI. PCI is not available within 120 minutes of first medical contact. After review of inclusion and exclusion criteria, the decision has been made to administer fibrinolytic therapy per the 2025 ACC/AHA ACS guideline.[1]
No absolute contraindications identified — ***
(no prior ICH / no known intracranial neoplasm or AVM / no active internal bleeding / no suspected aortic dissection / no significant head or facial trauma within 3 months / no ischemic stroke within 3 months).
Fibrinolytic administered: Tenecteplase *** mg IV bolus (weight-based: <60 kg = 30 mg, 60–69 kg = 35 mg, 70–79 kg = 40 mg, 80–89 kg = 45 mg, ≥90 kg = 50 mg).
Adjunctive therapy: ASA 325 mg, clopidogrel *** (300 mg if ≤75 years / 75 mg if >75 years), enoxaparin *** (30 mg IV bolus then 1 mg/kg SQ q12h if ≤75 years / no bolus, 0.75 mg/kg SQ q12h if >75 years).[1]
Reperfusion assessment at 60–90 minutes: *** (≥50% resolution of ST elevation suggests successful reperfusion / persistent ST elevation — arrange emergent transfer for rescue PCI).
Disposition: Transfer to PCI-capable facility for coronary angiography within 3–24 hours (pharmacoinvasive strategy).
Clinical Education
STEMI Criteria & Cath Lab Indications
STEMI is defined by new ST elevation at the J-point in ≥2 contiguous leads. The thresholds vary by lead and patient demographics:[2]
| Leads | Threshold |
| V2–V3 in men ≥40 years | ≥2 mm |
| V2–V3 in men <40 years | ≥2.5 mm (higher threshold due to benign early repolarization) |
| V2–V3 in women | ≥1.5 mm |
| All other leads | ≥1 mm |
| Posterior leads (V7–V9) | ≥0.5 mm |
Cath lab activation indications:[1]
| Indication | Details |
| Classic STEMI | STE meeting criteria in ≥2 contiguous leads with symptoms |
| STEMI equivalents | Posterior MI, de Winter, Wellens (type A), Sgarbossa-positive LBBB/paced, aVR STE with diffuse STD |
| Post-arrest STEMI | STEMI on post-ROSC ECG — emergent cath |
| Complicated NSTEMI | Hemodynamic instability, refractory ischemia, VT/VF, acute HF — urgent cath within 2 hours (Class 1A) |
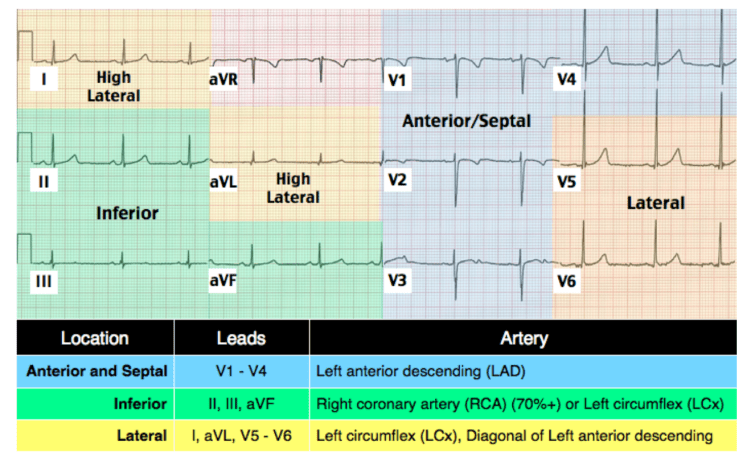
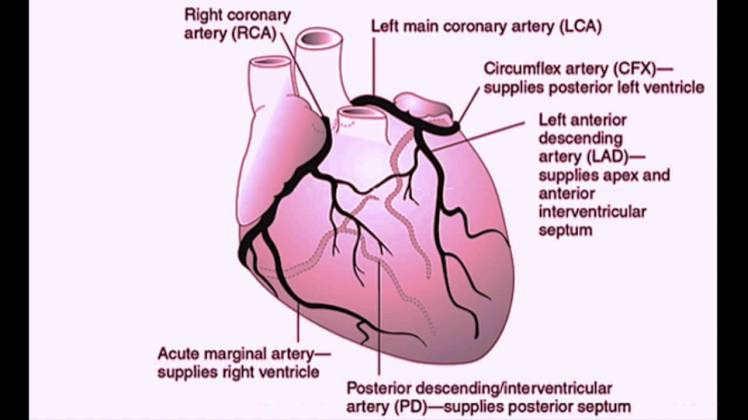
Territory and culprit artery:
| Territory | STE Leads | Reciprocal STD | Culprit |
| Anterior | V1–V4 (± V5–V6) | II, III, aVF | LAD |
| Inferior | II, III, aVF | I, aVL | RCA (85%) or LCx (15%) |
| Lateral | I, aVL, V5–V6 | III, aVF | LCx or diagonal branch of LAD |
| Posterior | V7–V9 (posterior leads) | STD V1–V3 with tall R, upright T | LCx or RCA (posterior descending) |
| Right ventricular | V4R (right-sided leads) | — | Proximal RCA |
STEMI Equivalents Deep Dive
These patterns represent acute coronary occlusion that does not meet traditional STEMI criteria on a standard 12-lead ECG. Missing these is one of the most consequential diagnostic errors in emergency medicine. See also: Hyperacute T Waves on the Chest Pain page.[3]
1. Posterior MI
ST depression in V1–V3 with tall R waves and upright T waves on a standard 12-lead represents posterior wall ischemia viewed as a “mirror image.” As Q waves develop on the posterior wall over hours, they appear as progressively tall R waves anteriorly — early on this can look like simple anteroseptal ischemia before the R waves form. Always obtain posterior leads (V7–V9) when you see isolated ST depression in V1–V3. Posterior STE > 0.5 mm confirms the diagnosis. Four percent of posterior MIs are isolated (no inferior STE), making them especially easy to miss.[3]
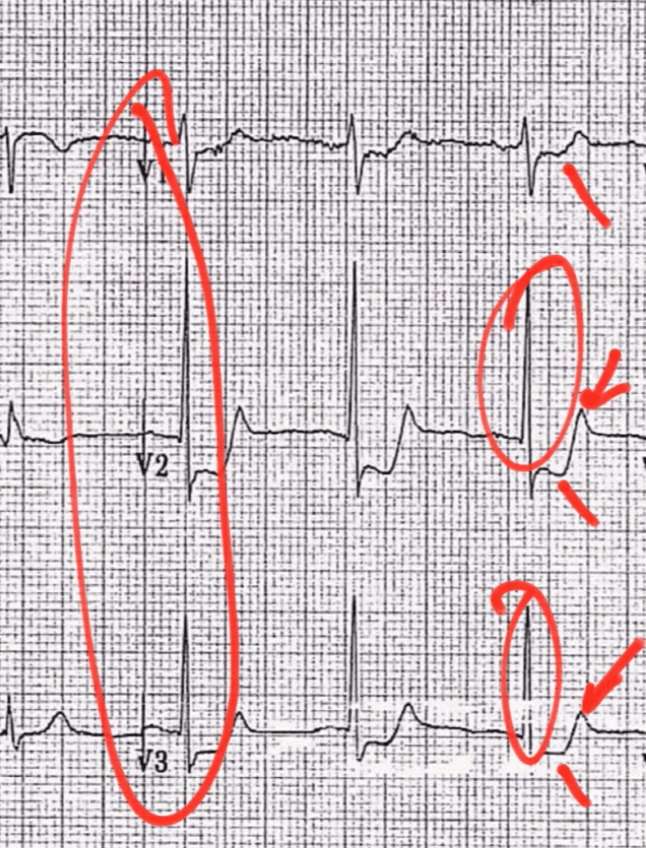
Posterior MI: STD V1–V3 with tall R waves — the mirror image of posterior STE.
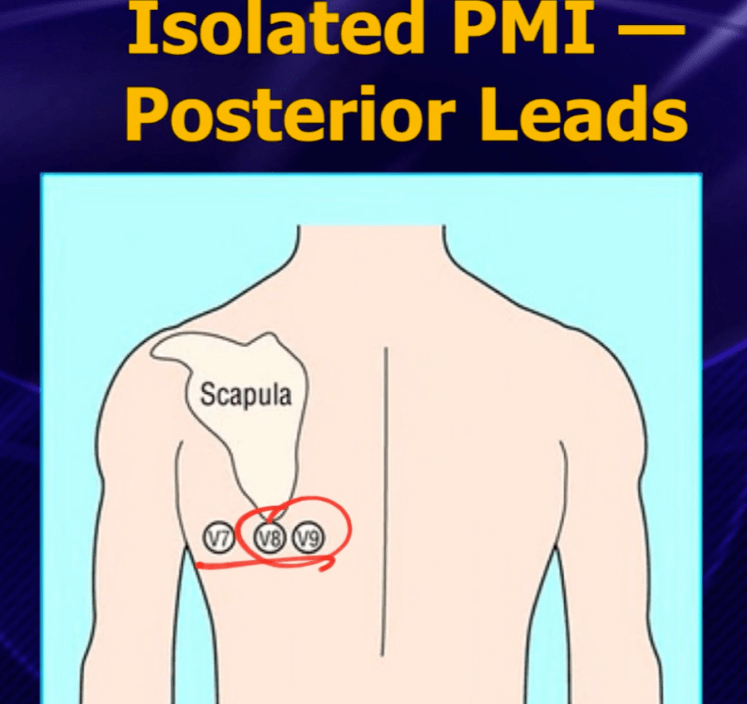
Posterior leads (V7–V9) revealing STE > 0.5 mm — confirming posterior STEMI.
2. De Winter T Waves
1–3 mm upsloping ST depression at the J-point in V1–V6 with tall, symmetric, peaked T waves. There is no ST elevation. This pattern represents acute LAD occlusion and is present in approximately 2% of anterior MIs. It is static — it does not evolve through the usual STEMI progression. Treat as LAD STEMI and activate the cath lab.[4]
3. Wellens Syndrome
Deeply inverted (Type A, 75%) or biphasic (Type B, 25%) T waves in V2–V3 (may extend to V1–V6) during a pain-free interval in a patient with recent chest pain. This represents a critical proximal LAD stenosis with reperfusion. Key: the ECG findings appear when the patient is NOT having pain. During active ischemia, the ECG may pseudo-normalize. Do NOT stress test — these patients need cath.[5]
4. Sgarbossa Criteria (LBBB / Paced Rhythm)
LBBB and ventricular paced rhythms make STEMI diagnosis on ECG extremely difficult because they produce expected discordant ST changes. The original Sgarbossa criteria and the modified Sgarbossa (Smith) criteria help identify acute MI in this setting:[6]
| Criterion | Original Sgarbossa | Modified (Smith) |
| Concordant STE ≥1 mm | 5 points (most specific) | Same — most specific finding |
| Concordant STD ≥1 mm in V1–V3 | 3 points | Same |
| Discordant STE | ≥5 mm (1 point) — poor sensitivity | STE/S-wave ratio ≥ 0.25 — significantly better sensitivity |
Use the modified (Smith) criteria. Any single positive criterion is sufficient to activate the cath lab. The modification of the third criterion (replacing the fixed 5 mm threshold with a proportional ratio of ≥0.25 relative to the preceding S-wave depth) dramatically improved sensitivity without sacrificing specificity.[6]
Key pearl: The 2025 ACS guideline states that new or presumably new LBBB alone is no longer considered a STEMI equivalent. LBBB requires Sgarbossa criteria to be met for cath lab activation.[1]
5. aVR ST Elevation
In a sick patient with acute chest pain, aVR STE > 1 mm with diffuse ST depression (especially in lateral leads) suggests left main coronary artery occlusion or severe triple-vessel disease — mortality may approach 70%. Two criteria must be met: the patient looks sick AND there is diffuse STD in other leads. In a well-appearing patient, the same pattern may be seen with SVT, atrial fibrillation with RVR, LBBB, LVH, or pacemaker rhythm and is not an activation.[7]
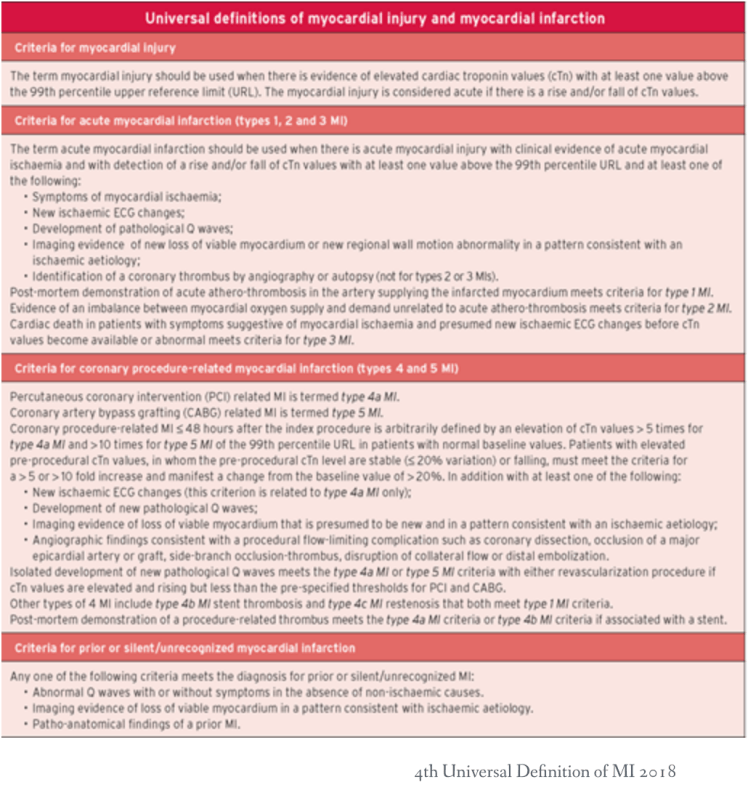
From the 4th Universal Definition of MI (ESC/ACC/AHA/WHF, 2018).
Right Ventricular MI Pearls
Up to 40% of inferior MIs involve the right ventricle. RV MI changes management significantly and must be identified early. Obtain right-sided leads (particularly V4R) on every inferior STEMI — STE ≥1 mm in V4R has ~90% sensitivity and specificity for RV involvement.[8]
The RV is preload-dependent and afterload-sensitive. When the RV fails, forward flow into the left heart drops, causing hypotension. The treatment principles are the opposite of LV failure:
| Do | Do NOT |
| Aggressive IV fluid resuscitation (1–2 L NS bolus) | Nitroglycerin — can cause precipitous hypotension by reducing preload |
| Target MAP > 65 with fluids first | Morphine — venodilator, reduces preload |
| Dobutamine if fluids fail (inotropic support) | Diuretics — further reduce preload |
| Early reperfusion (PCI is definitive treatment) | High PEEP if intubated — increases RV afterload |
Clinical triad of RV MI: Hypotension + elevated JVP + clear lung fields (no pulmonary edema despite cardiogenic shock). This distinguishes RV MI from LV failure, which presents with pulmonary congestion.[8]
ECG pearl: RV MI can also manifest as STE in V1 in the setting of inferior STEMI. If you see inferior STE with STE in V1 (and not V2), think RV involvement and get right-sided leads.[3]
ED STEMI Medications
The goal is rapid dual antiplatelet therapy + anticoagulation before the patient reaches the cath lab. The 2025 ACC/AHA ACS guideline provides updated recommendations:[1]
| Category | Agent | Dose | Notes |
| Aspirin | Non-enteric coated ASA | 162–325 mg PO (chewed) | Give immediately. Class 1. |
| P2Y12 inhibitor | Ticagrelor (preferred) | 180 mg PO loading dose | Faster onset, more potent, reversible. Avoid if prior ICH or on dialysis. Contraindication: oral anticoagulant use. |
| Clopidogrel | 600 mg PO loading dose | If ticagrelor contraindicated. Slower onset. 300 mg if giving with fibrinolytics (≤75 yrs). No loading if >75 yrs with fibrinolytics. | |
| Anticoagulation | UFH (for primary PCI) | Bolus 60 U/kg (max 4,000 U), gtt 12 U/kg/hr (max 1,000 U/hr) | Standard for cath lab pathway. Titrate to ACT in lab. |
| Enoxaparin (for fibrinolytic pathway) | ≤75 yrs: 30 mg IV bolus + 1 mg/kg SQ q12h >75 yrs: No bolus, 0.75 mg/kg SQ q12h CrCl <30: 1 mg/kg SQ q24h |
Preferred over UFH when giving fibrinolytics. | |
| Analgesia | Fentanyl | 25–50 mcg IV PRN | Preferred over morphine. See below. |
Timing pearl: Discuss P2Y12 choice with the interventionalist before loading if possible — some prefer to wait until coronary anatomy is known (in case CABG is needed, as ticagrelor delays surgery by 5 days and clopidogrel by 7 days). In practice, most STEMI patients get loaded in the ED.[1]
Morphine & Oxygen — What NOT to Give
Morphine: Multiple studies have raised concern about morphine in ACS. Morphine delays gastric emptying and slows absorption of oral P2Y12 inhibitors, leading to delayed antiplatelet effect and increased platelet reactivity.[9] In NSTEMI patients, morphine use has been associated with higher mortality in observational data.[10] The 2025 ACS guideline does not recommend routine morphine for ACS pain. Use fentanyl instead — its adverse interactions with antiplatelet agents have not been demonstrated, and it provides equivalent analgesia.[1]
Oxygen: The AVOID trial (2015) demonstrated that supplemental oxygen in STEMI patients without hypoxia was associated with larger infarct size, more recurrent MI, and more arrhythmias at 6 months.[11] The DETO2X-AMI trial (2017) confirmed no benefit of routine O2 in MI patients with SpO2 ≥90%.[12] Only give oxygen if SpO2 < 90%.
Diabetic “painless MI”: Diabetic patients may have autonomic neuropathy causing decreased cardiac sensory innervation, leading to atypical or absent chest pain. Maintain a high index of suspicion for ACS in diabetics presenting with dyspnea, diaphoresis, nausea, or unexplained hemodynamic instability — and get an ECG early.[13]
Post-Arrest STEMI
STEMI on post-ROSC ECG = emergent cath lab activation. This is a Class 1 recommendation in the 2025 ACS guideline.[1]
Post-arrest NSTEMI / no STEMI on ECG: The decision is more nuanced. The 2025 guideline recommends coronary angiography within 2 hours for post-arrest patients with a high suspicion for ACS as the cause of arrest (e.g., preceding chest pain, known CAD, shockable rhythm) even without STEMI on ECG. For patients without obvious cardiac etiology or with clearly non-cardiac causes of arrest, emergent angiography may be deferred while other workup is pursued.[1]
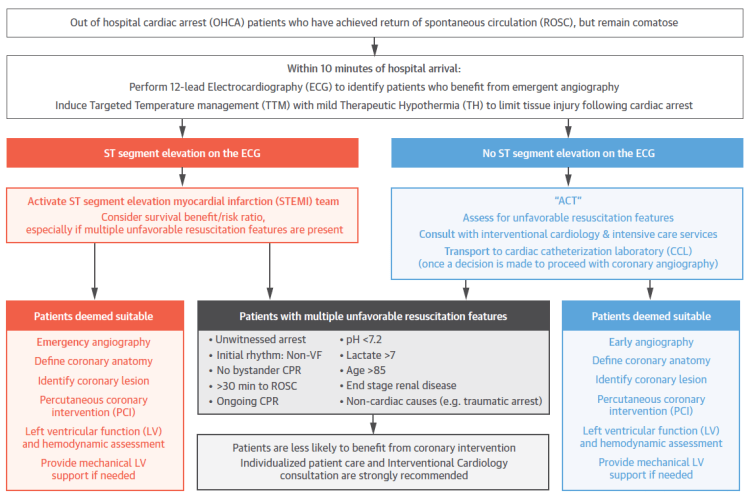
Interventional Council, ACC 2015 algorithm for comatose post-ROSC patients — still useful framework, though the 2025 ACS guideline has updated specific recommendations.
Cardiogenic Shock Recognition
Cardiogenic shock complicates 5–8% of STEMIs and carries 40–50% mortality. Early recognition and escalation is critical.[14]
Clinical definition: Sustained SBP < 90 mmHg (or vasopressors required to maintain SBP ≥90) with evidence of end-organ hypoperfusion — altered mental status, cool/mottled extremities, oliguria, or rising lactate.
ED management:
| Intervention | Details |
| Reperfusion | Emergent PCI — the most important intervention. Do not delay for stabilization. |
| Vasopressor | Norepinephrine first-line (SOAP II trial showed lower mortality vs dopamine in cardiogenic shock).[15] |
| Inotrope | Dobutamine 2–20 mcg/kg/min if low cardiac output with adequate MAP. Milrinone as alternative. |
| Mechanical support | Discuss with interventionalist early: IABP, Impella, or ECMO may be placed in the cath lab. |
| Avoid | Excessive fluids (may worsen pulmonary edema), beta-blockers, nitrates in hypotension. |
Mechanical complications to consider (typically days 3–7 post-MI but can present earlier): ventricular septal rupture (new harsh systolic murmur), free wall rupture (tamponade), acute mitral regurgitation from papillary muscle rupture (acute pulmonary edema with new murmur). All require emergent surgical consultation.[14]
References
- Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes. Circulation. 2025. AHA Journals
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018;138(20):e618–e651. PubMed
- Burns E, Buttner R. STEMI — ECG Library. Life in the Fast Lane. 2021. LITFL
- de Winter RJ, Verouden NJ, Wellens HJ, Wilde AA. A new ECG sign of proximal LAD occlusion. N Engl J Med. 2008;359(19):2071–2073. PubMed
- Rhinehardt J, Brady WJ, Perron AD, Mattu A. Electrocardiographic manifestations of Wellens’ syndrome. Am J Emerg Med. 2002;20(7):638–643. PubMed
- Smith SW, Dodd KW, Henry TD, et al. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med. 2012;60(6):766–776. PubMed
- Kosuge M, Ebina T, Hibi K, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol. 2011;107(4):495–500. PubMed
- Ondrus T, Kanovsky J, Novotny T, et al. Right ventricular myocardial infarction: from pathophysiology to prognosis. Exp Clin Cardiol. 2013;18(1):27–30. PubMed
- Kubica J, Adamski P, Ostrowska M, et al. Morphine delays and attenuates ticagrelor exposure and action in patients with myocardial infarction: the randomized, double-blind, placebo-controlled IMPRESSION trial. Eur Heart J. 2016;37(3):245–252. PubMed
- Meine TJ, Roe MT, Chen AY, et al. Association of intravenous morphine use and outcomes in acute coronary syndromes. Am Heart J. 2005;149(6):1043–1049. PubMed
- Stub D, Smith K, Bernard S, et al. Air Versus Oxygen in ST-Segment-Elevation Myocardial Infarction (AVOID). Circulation. 2015;131(24):2143–2150. PubMed
- Hofmann R, James SK, Jernberg T, et al. Oxygen Therapy in Suspected Acute Myocardial Infarction (DETO2X-AMI). N Engl J Med. 2017;377(13):1240–1249. PubMed
- Umachandran V, Ranjadayalan K, Ambepityia G, et al. The perception of angina in diabetes: relation to somatic pain threshold and autonomic function. Am Heart J. 1991;121(6 Pt 1):1649–1654. PubMed
- van Diepen S, Katz JN, Albert NM, et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the AHA. Circulation. 2017;136(16):e52–e68. PubMed
- De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine and norepinephrine in the treatment of shock (SOAP II). N Engl J Med. 2010;362(9):779–789. PubMed
