Last reviewed: March 2026
Contents
MDM Templates
Vasovagal / Reflex Syncope
Patient presents after a syncopal episode with a clear prodrome (lightheadedness, warmth, diaphoresis, nausea) and identifiable trigger (prolonged standing, pain, emotional stress). Rapid return to baseline with no confusion or postictal state. No exertional component. No chest pain, palpitations, or dyspnea preceding the event.
History classic for vasovagal syncope — prodromal symptoms with identifiable trigger, brief LOC, and rapid recovery. ECG shows no evidence of Brugada pattern, delta wave, epsilon wave, prolonged QTc, or dysrhythmia. Not consistent with cardiac syncope (prodrome present, no exertional component, normal ECG), seizure (no tonic-clonic activity, no postictal state, no tongue bite), or orthostatic hypotension (not positional alone, triggered by specific stimulus).
Plan: Discharge with PCP follow-up. Return for recurrent syncope, exertional syncope, palpitations, chest pain, or syncope without warning.
Syncope — Cardiac Concern
Patient presents after a syncopal episode with features concerning for cardiac etiology — no prodrome, exertional onset, associated palpitations or chest pain, or family history of sudden cardiac death. No clear vasovagal trigger.
Absence of prodrome and presence of concerning features raise suspicion for cardiac syncope. Differential includes dysrhythmia (VT, SVT with rapid rate, bradydysrhythmia, heart block), structural heart disease (HOCM, aortic stenosis), and conduction system disease (Brugada, long QT, WPW). Not consistent with vasovagal syncope (no prodrome, no trigger) or seizure (no postictal state).
If ECG abnormal: ECG demonstrates findings concerning for conduction abnormality. Cardiology consulted regarding further workup and disposition.
Plan: Admit to telemetry for cardiac monitoring. Cardiology consulted.
Clinical Education
Approach to Syncope in the ED
The ED job is to find dangerous causes, not to diagnose every syncope. Most syncope is vasovagal and benign. The dangerous causes are cardiac — dysrhythmia, structural heart disease, and conduction abnormalities. History and ECG are the two most important tools. Everything else (troponin, CT head, echo) is low yield unless the history or ECG directs you there.[1]
History features that point to cardiac syncope: no prodrome (sudden LOC without warning), exertional syncope, syncope while supine, preceding palpitations or chest pain, family history of sudden cardiac death under age 50. Any of these should lower your threshold for admission and workup.
History features that point to benign syncope: clear prodrome (lightheadedness, warmth, tunnel vision, nausea), identifiable trigger (prolonged standing, pain, blood draw, Valsalva), rapid return to baseline, and young age without cardiac history.
Don’t CT every syncope. Head CT is indicated if there was head trauma from the fall, the patient is anticoagulated with head trauma, or there are focal neurologic deficits suggesting stroke. Routine head CT for uncomplicated syncope has extremely low yield.[2]
Dangerous ECG Findings
Every syncope patient gets an ECG. The following findings require admission and cardiology evaluation:
| Finding | Concern | Key Features |
| Brugada pattern | Polymorphic VT → VF → sudden death | Coved or saddleback STE in V1–V2 with incomplete RBBB pattern. Type 1 (coved) is diagnostic; Type 2 (saddleback) needs EP evaluation. Can be unmasked by fever or Na+ channel blockers. |
| Delta wave (WPW) | Accessory pathway → reentrant tachycardia or AF with rapid conduction | Short PR with slurred upstroke of QRS. Dangerous if AF develops — can degenerate to VF. |
| Prolonged QTc | Torsades de pointes | QTc >500 ms is high risk. Can be congenital or acquired (drugs, electrolytes). Review medication list. |
| Epsilon wave | Arrhythmogenic right ventricular cardiomyopathy (ARVC) | Small notch at the end of QRS in V1–V3. At risk for VT. Needs ICD evaluation. |
| High-degree AV block | Bradycardia-related syncope | Mobitz II or third-degree block. May need pacing. |
| VT or sustained SVT | Tachyarrhythmia-related syncope | Wide complex tachycardia = VT until proven otherwise. |
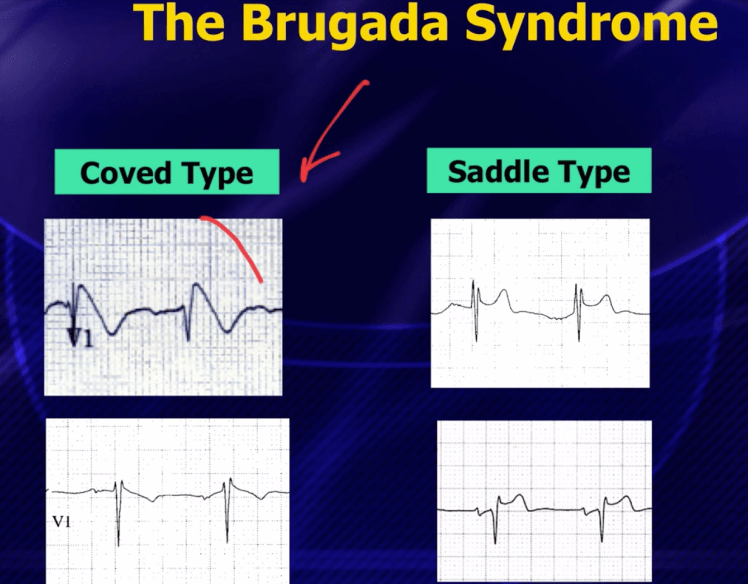
If you see a Brugada pattern that resolves (e.g., unmasked by fever and resolves when afebrile), the patient still needs admission for inpatient electrophysiology evaluation. A transient Brugada pattern is still a Brugada substrate. Consider placing V1 and V2 one intercostal space higher if the pattern is borderline — this can unmask it.[3]
Risk Stratification
High-risk features that warrant admission: abnormal ECG, exertional syncope, syncope while supine, no prodrome, associated chest pain or dyspnea, family history of sudden death <50, known structural heart disease, new murmur, age >60 with no clear benign cause, significant injury from the event.
Low-risk features supporting discharge: classic vasovagal history with prodrome and trigger, young patient with no cardiac history, normal ECG, no injury, rapid return to baseline, and prior similar episodes with benign evaluation.
The San Francisco Syncope Rule (CHESS) and Canadian Syncope Risk Score exist for risk stratification, but neither is sensitive enough to replace clinical judgment. Use them as frameworks, not as stand-alone decision tools. The Canadian Syncope Risk Score has the best validation data and predicts 30-day serious adverse events.[4]
Don’t check troponin on every syncope. It’s indicated if the patient has chest pain, dyspnea, ECG changes, or other features suggesting ACS. A young person with a classic vasovagal episode does not need cardiac biomarkers.[2]
Disposition
Discharge: Classic vasovagal or reflex syncope with identifiable trigger, normal ECG, normal neurologic exam, and return to baseline. Ensure PCP follow-up. Counsel on avoidance of triggers and prodromal awareness (sit or lie down when symptoms start).
Admit to telemetry: Abnormal ECG, exertional or supine syncope, no prodrome with concerning features, known structural heart disease, significant dysrhythmia, or any patient where cardiac etiology cannot be excluded. Telemetry is the key intervention — catching an arrhythmia on monitoring is the diagnostic yield of admission.
Consider admission for: Elderly patients with no clear cause (even if ECG is normal), patients with significant injury from the fall who need observation, and patients with recurrent unexplained syncope who may benefit from expedited inpatient workup.
References
- Brignole M, Moya A, de Lange FJ, et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):1883-1948. PubMed
- Huff JS, Decker WW, Quinn JV, et al. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with syncope. Ann Emerg Med. 2007;49(4):431-444. PubMed
- Antzelevitch C, Brugada P, Borggrefe M, et al. Brugada syndrome: report of the second consensus conference. Circulation. 2005;111(5):659-670. PubMed
- Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope. CMAJ. 2016;188(12):E289-E298. PubMed
