Last reviewed: March 2026
Contents
MDM Templates
Cyanotic Neonate — Duct-Dependent Lesion
Neonate presents with cyanosis unresponsive to supplemental oxygen. Well or ill appearing with oxygen saturations that do not improve with 100% FiO2. Pre- and post-ductal saturations obtained. No respiratory distress to suggest primary pulmonary pathology.
Presentation concerning for duct-dependent congenital heart disease. Differential includes tetralogy of Fallot, transposition of the great arteries, truncus arteriosus, total anomalous pulmonary venous return, tricuspid atresia, hypoplastic left heart syndrome, critical coarctation, and critical pulmonary or aortic stenosis. Sepsis, pneumonia, methemoglobinemia, and foreign body aspiration also considered but less consistent with this presentation.[1]
Plan: Prostaglandin E1 initiated at 0.05 mcg/kg/min. Pediatric cardiology consulted regarding echocardiography and definitive management. Prepared for potential apnea and hypotension from PGE1 — intubation equipment at bedside.
Disposition: Admit to PICU. Transfer to pediatric cardiac surgery center if not available on site.
Tet Spell
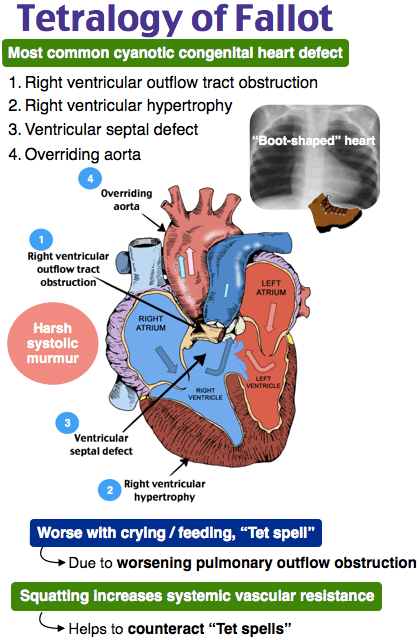
Infant with known or newly suspected tetralogy of Fallot presents with acute cyanotic episode. Child was crying and became deeply cyanotic with increased respiratory effort.
Presentation consistent with hypercyanotic (“tet”) spell from dynamic right ventricular outflow tract obstruction causing increased right-to-left shunting. Not consistent with sepsis, pneumonia, foreign body aspiration, or arrhythmia based on history and exam.[2]
Plan: Knee-to-chest positioning. Supplemental oxygen. Morphine 0.1 mg/kg IV for anxiolysis and pulmonary vasodilation. IV fluid bolus 10 mL/kg to increase preload. Pediatric cardiology consulted.
If refractory: Phenylephrine 5-10 mcg/kg IV bolus to increase SVR. Ketamine 1 mg/kg IM/IV for sedation and SVR augmentation. Consider esmolol infusion if persistent dynamic RVOT obstruction.[2]
Disposition: Admit to PICU for monitoring and surgical planning.
Acyanotic CHD — Heart Failure
Infant presents with poor feeding, diaphoresis with feeds, and failure to gain weight. Tachycardic, tachypneic, with hepatomegaly on exam. Murmur appreciated.
Presentation concerning for heart failure from acyanotic congenital heart disease, most commonly a left-to-right shunt lesion (VSD, ASD, PDA, AV canal defect). As pulmonary vascular resistance drops in the weeks after birth, increasing left-to-right flow leads to pulmonary overcirculation and heart failure. Sepsis, metabolic disorder, and pneumonia also considered.[1]
Plan: IV access, monitor, CXR. Pediatric cardiology consulted for echocardiography. Diuresis if volume overloaded. Careful with IV fluids — avoid volume overload in a failing heart.
Disposition: Admit for echocardiography, cardiology evaluation, and hemodynamic monitoring.
Clinical Education
Cyanotic vs Acyanotic Lesions
Cyanotic lesions (right-to-left shunt) present early — often in the first days to weeks of life as the ductus arteriosus closes. The “5 T’s”: Tetralogy of Fallot, Transposition of the Great Arteries, Truncus Arteriosus, Total Anomalous Pulmonary Venous Return, Tricuspid Atresia.[1]
Acyanotic lesions (left-to-right shunt) present later — typically at 4-8 weeks as pulmonary vascular resistance falls and the shunt increases. VSD is the most common congenital heart defect overall. ASD, PDA, and AV canal defects also present with pulmonary overcirculation and eventual heart failure.
Ductal-dependent lesions are the immediate emergencies. Any cyanotic neonate in the first weeks of life who doesn’t improve with oxygen should be presumed to have duct-dependent CHD until proven otherwise.
The Hyperoxia Test
Place the infant on 100% FiO2 for 10 minutes and obtain an ABG. If the PaO2 remains below 100 mmHg, the infant has a fixed right-to-left shunt — this is congenital heart disease until proven otherwise.[1]
Pre- and post-ductal saturations add further information. Right hand = pre-ductal, either foot = post-ductal. A difference >3% suggests a ductal-level shunt (coarctation, interrupted aortic arch, or PPHN).
A normal hyperoxia test does not completely exclude CHD — some lesions with mixing physiology (truncus, large VSD) may partially improve with oxygen. Clinical suspicion should drive the echo.
Prostaglandin E1
Start PGE1 at 0.05 mcg/kg/min for any neonate <4 weeks with suspected duct-dependent CHD. This reopens or maintains the ductus arteriosus, buying time for definitive diagnosis and surgical planning.[3]
Key adverse effects: apnea (12%) and hypotension. Have intubation equipment at bedside before starting. Consider elective intubation before transport if the infant will be transferred.
Do not withhold PGE1 while waiting for echo confirmation. In a cyanotic neonate failing the hyperoxia test, the risk of NOT starting PGE1 far outweighs the side effects. Start it and let cardiology sort out the anatomy.
Tet Spell Management
The pathophysiology is dynamic RVOT obstruction → increased R-to-L shunt → cyanosis. The treatment ladder targets reducing the obstruction and increasing systemic vascular resistance to push blood through the lungs.[2]
| Step | Intervention | Mechanism |
| 1 | Knee-to-chest positioning | Increases SVR (compresses femoral arteries) |
| 2 | Oxygen, calm environment | Decreases PVR, reduces agitation |
| 3 | Morphine 0.1 mg/kg IV | Anxiolysis, may decrease PVR |
| 4 | IV fluid bolus 10 mL/kg | Increases preload and pulmonary blood flow |
| 5 | Phenylephrine 5-10 mcg/kg IV | Increases SVR → reverses shunt |
| 6 | Ketamine 1 mg/kg IM/IV | Increases SVR + sedation |
| 7 | Esmolol infusion | Relaxes RVOT spasm directly |
Avoid agitating the child. Blood draws, IV starts, and crying all worsen the spell. Sedate first, then access.
Heart Failure in Infants
Heart failure in infants looks like poor feeding, not ankle edema. Classic signs: diaphoresis with feeds, tachypnea, tachycardia, hepatomegaly, and failure to gain weight. Parents often describe the infant “working hard to eat” or taking 45+ minutes per feed.[1]
CXR may show cardiomegaly and pulmonary vascular congestion. This helps distinguish cardiac from pulmonary causes of tachypnea.
Be cautious with IV fluids. These infants are volume overloaded from pulmonary overcirculation. A bolus for “dehydration” can push them into acute pulmonary edema. If the infant needs volume, give small aliquots (5 mL/kg) and reassess.
Disposition Decision Guide
Immediate PICU / transfer to cardiac surgery center: Any cyanotic neonate on PGE1. Any tet spell requiring pharmacologic intervention beyond positioning. Any infant in decompensated heart failure.
Admit to pediatrics: New murmur with heart failure symptoms but hemodynamically stable. Infant needing echo and cardiology evaluation but not in acute distress.
Discharge with close follow-up (rare from ED): Incidentally discovered asymptomatic murmur in a well-appearing, well-growing child with normal saturations. Outpatient echo and cardiology referral within 1-2 weeks. Return if poor feeding, cyanosis, or increased work of breathing.
References
- Stout KK, Daniels CJ, Perloff RK, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease. Circulation. 2019;139(14):e698-e800. PubMed
- Bailliard F, Anderson RH. Tetralogy of Fallot. Orphanet J Rare Dis. 2009;4:2. PubMed
- Mazur A, Trefler R, Jaber S. Prostaglandin E1 in the management of duct-dependent congenital heart disease. Paediatr Drugs. 2022;24(2):103-112. PubMed
