Last reviewed: March 2026
Contents
MDM Templates
Prepubertal Bleeding — Benign Etiology
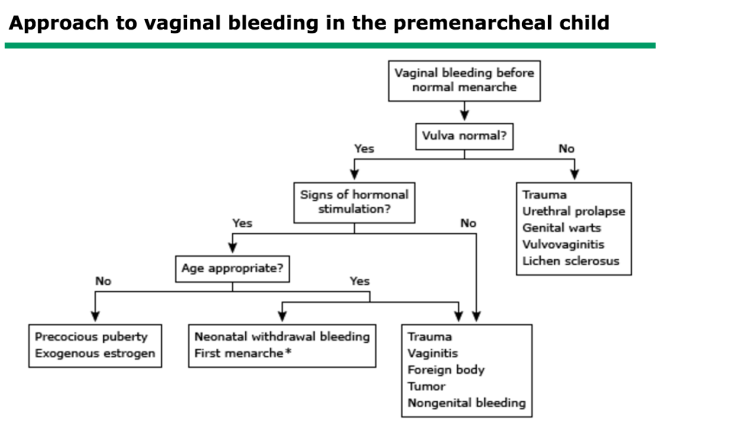
Prepubertal female presents with genital bleeding. External exam reveals source consistent with benign etiology — straddle injury with labial laceration, vulvar irritation, or urethral prolapse. No signs of penetrating trauma. No foreign body visualized. No signs of hormonal stimulation or precocious puberty.
History is consistent and age-appropriate for the mechanism described. Story is linear between child and caregivers. Low concern for inflicted injury or sexual abuse at this time. Not consistent with vaginal foreign body (no foul-smelling discharge), tumor (no mass), or hormonal pathology (no breast development or pubic hair).[1]
Plan: Local wound care. Sitz baths for comfort. Discharge with PCP follow-up. Return for recurrent bleeding, foul-smelling discharge, pain with urination, or signs of infection.
Prepubertal Bleeding — Abuse Concern
Prepubertal female presents with genital bleeding with features raising concern for sexual abuse — history inconsistent with exam findings, penetrating injury pattern, hymenal laceration, STI in prepubertal child, or behavioral indicators (regression, sexualized behavior).
Exam findings and clinical context raise concern for inflicted injury. Vaginal bleeding in a prepubertal child with penetrating trauma pattern is abuse until proven otherwise. Not consistent with accidental straddle injury (which typically involves external labial/periurethral structures, not the hymen or vagina).[2]
Plan: Exam performed with attention to documentation (describe findings objectively, use clock-face positioning for hymenal injuries). If acute assault (<72 hours), forensic evidence collection per institutional protocol. STI testing. Social work and child protective services notified. Admit if surgical repair needed or if safe discharge environment is not available.
Adolescent Vaginal Bleeding
Adolescent female presents with vaginal bleeding. Hemodynamically stable. Pregnancy test negative. No signs of hemodynamic compromise.
Most common cause of abnormal vaginal bleeding in adolescents is anovulatory (dysfunctional uterine) bleeding due to immature hypothalamic-pituitary-ovarian axis. Differential also includes pregnancy complications (despite negative POC — consider very early pregnancy or ectopic), coagulopathy (especially if heavy menses since menarche), infection, and trauma. Not consistent with ectopic pregnancy, miscarriage, or hemorrhagic ovarian cyst based on current evaluation.[1]
Plan: Treat based on severity. Mild: reassurance and PCP/GYN follow-up. Moderate: hormonal therapy initiated. Severe (hemodynamic compromise or Hgb <7): IV estrogen, transfusion, GYN consultation. Discharge with follow-up. Return for heavy bleeding soaking >1 pad per hour, dizziness, or syncope.
If pregnancy test positive with vaginal bleeding: Quantitative beta-hCG, type and screen, Rh status. Pelvic ultrasound to evaluate for intrauterine pregnancy, ectopic, or retained products. OB/GYN consulted. RhoGAM if Rh-negative.
Clinical Education
DDx by Age
| Age Group | Common Causes |
| Neonate | Estrogen withdrawal (physiologic — normal response to maternal hormones) |
| Prepubertal (2-8 yr) | Vulvovaginitis, foreign body, straddle injury, urethral prolapse, lichen sclerosus, sexual abuse, tumor (rare) |
| Perimenarchal / Adolescent | Anovulatory bleeding (DUB), pregnancy complications, coagulopathy, infection (cervicitis, PID), ovarian cyst, trauma |
Prepubertal Bleeding Pearls
Vaginal foreign body is the most common cause of foul-smelling bloody discharge in prepubertal girls. Small pieces of toilet paper are the most frequent foreign body. Diagnosis is often made on exam or with vaginoscopy under sedation if foreign body is suspected but not visualized externally.[1]
Urethral prolapse presents as a “donut” of dark red or purple tissue around the urethral meatus. It is idiopathic and more common in African American girls. Treatment is conservative (sitz baths, topical estrogen cream). Surgery is rarely needed.
Hymenal laceration from straddle injury is uncommon. Straddle injuries typically cause labial, periurethral, or perineal contusions and lacerations — they do not typically cause hymenal or vaginal injuries. Hymenal tears or vaginal lacerations should raise concern for penetrating trauma and possible abuse.[2]
Genital warts (condylomata acuminata) in children <4 years may be acquired by vertical transmission and do not automatically indicate abuse. In children >4 years, genital warts warrant evaluation for sexual abuse and CPS notification.
Bloody vaginal discharge in a neonate in the first 1-2 weeks of life is a normal physiologic response to withdrawal of maternal estrogen. No workup or treatment needed. Reassure family.
Adolescent Bleeding Pearls
Anovulatory bleeding accounts for the majority of abnormal uterine bleeding in the first 2 years after menarche. The immature HPO axis produces estrogen without regular ovulation, leading to unopposed estrogen stimulation of the endometrium with irregular, sometimes heavy shedding. Most cases resolve spontaneously as the axis matures.[1]
Screen for coagulopathy in any adolescent with heavy menstrual bleeding since menarche. Up to 20% of adolescents hospitalized for menorrhagia have an underlying bleeding disorder, most commonly von Willebrand disease. Obtain CBC, PT/INR, PTT, fibrinogen, and von Willebrand panel.
Always obtain a pregnancy test regardless of stated sexual history. Ectopic pregnancy, threatened/incomplete abortion, and molar pregnancy all present with vaginal bleeding. A negative urine pregnancy test with clinical suspicion warrants quantitative serum beta-hCG (urine can be falsely negative very early).
Sexual Abuse Evaluation
A normal genital exam does not exclude sexual abuse. The majority of sexually abused children have completely normal exams, particularly if the abuse was non-penetrating or the exam is delayed. The child’s history is the most important diagnostic element.[2]
Findings highly specific for abuse: acute hymenal lacerations (especially posterior), genital bruising inconsistent with straddle mechanism, presence of semen, and STIs in prepubertal children (gonorrhea, chlamydia, syphilis, HIV are diagnostic of abuse in this age group).
Forensic evidence collection is indicated within 72 hours of acute assault (some protocols extend to 96 hours). Use institutional forensic kits. Document all findings with clinical photos when possible. Interview the child separately from caregivers using open-ended, non-leading questions — or defer the forensic interview to a trained child advocacy center.
Mandatory reporting applies in all cases of suspected abuse. The physician’s legal obligation is to report reasonable suspicion, not to prove abuse occurred.
Disposition
Admit: Hemodynamically significant bleeding requiring transfusion or IV estrogen. Vaginal laceration requiring surgical repair under anesthesia. Suspected abuse without safe discharge environment. Ectopic pregnancy.
Discharge: Benign prepubertal bleeding (straddle injury, vulvovaginitis, urethral prolapse) with PCP follow-up. Anovulatory bleeding that is hemodynamically stable with outpatient GYN follow-up arranged. Threatened abortion with stable vital signs and reliable OB follow-up. Return for heavy bleeding, dizziness, abdominal pain, fever, or foul-smelling discharge.
References
- Emans SJ, Laufer MR. Emans, Laufer, Goldstein’s Pediatric and Adolescent Gynecology. 7th ed. Wolters Kluwer; 2020. Publisher
- Jenny C, Crawford-Jakubiak JE, Committee on Child Abuse and Neglect, AAP. The evaluation of children in the primary care setting when sexual abuse is suspected. Pediatrics. 2013;132(2):e558-e567. PubMed
