Last reviewed: March 2026Contents
MDM Templates
VP Shunt Malfunction
Patient with VP shunt presents with headache, nausea, and vomiting — symptoms consistent with shunt malfunction. No fever, no erythema along the shunt tract, no altered mentation. Neurologic exam at baseline.
Symptoms are consistent with the patient’s prior shunt malfunction episodes. Shunt obstruction is the most common cause. Low suspicion for shunt infection given absence of fever and tract erythema. Not consistent with migraine (pattern matches prior malfunctions, not typical migraine history) or other intracranial pathology given known shunt dependence.
If findings of obstruction/malfunction and neurosurgery consulted:
Neurosurgery consulted regarding imaging findings, shunt function, and need for operative intervention.
Plan: Shunt series and brain imaging obtained. Neurosurgery consulted. Admit for observation and shunt evaluation.
VP Shunt Infection
Patient with VP shunt presents with headache and fever. Exam notable for tenderness or erythema along the shunt tract. This raises concern for shunt infection.
Shunt infection carries high morbidity and typically requires shunt externalization and IV antibiotics. Most infections occur within 6 months of placement and are caused by skin flora (Staphylococcus epidermidis most common). Not consistent with simple viral illness given tract findings. Meningitis also considered but shunt infection is the more likely source in this context.
Plan: Neurosurgery consulted for shunt tap and CSF analysis. Empiric antibiotics initiated after CSF obtained. Admit.
Clinical Education
Approach to VP Shunt Problems
VP shunt patients who present with headache, nausea, or vomiting should be assumed to have a shunt problem until proven otherwise. These are shunt-dependent patients — their baseline neurologic function relies on the shunt working. The two main categories are malfunction (obstruction, disconnection, migration) and infection.[1]
Ask the patient (or caregiver): What type of shunt do you have? When was it placed or last revised? What did your prior malfunction feel like? Does this feel the same? These patients are experts on their own shunt failures — if they tell you it feels like their last malfunction, believe them.
Imaging Pitfalls
Imaging misses up to one-third of shunt malfunctions. Ventricle size on CT can be misleading — “small ventricles stay small, big ventricles stay big.” Patients with chronically small, noncompliant ventricles can have large changes in ICP without visible changes in ventricle size. Always compare to the patient’s baseline imaging if available.[2]
Shunt series (skull, chest, abdomen X-rays) evaluates for mechanical problems — disconnection, kinking, migration of the distal catheter. It does not tell you if the shunt is flowing.
Fast T2 MRI (a single T2 sequence, takes <15 seconds) is increasingly used for rapid ventricle assessment without radiation. Useful for comparison to baseline in patients with frequent ED visits.
A normal CT does not rule out malfunction. If the clinical picture is consistent with malfunction and imaging is unremarkable, consult neurosurgery anyway.
Overshunting vs Undershunting
Overshunting (overdrainage) is actually the most common cause of headache in shunt patients. Headaches from overshunting are typically worse when upright and improve with lying down (low-pressure headache, similar to post-LP headache). The ventricles will appear slit-like on imaging.
Undershunting (obstruction) presents with headaches that are worse in the morning — hypoventilation during sleep increases CO2, causing cerebral vasodilation and increased ICP. The ventricles may or may not be enlarged depending on compliance.
The key distinction is positional: worse upright = overshunting, worse supine/morning = undershunting. This helps guide the neurosurgery conversation about valve pressure adjustment vs surgical revision.
Shunt Infection Pearls
80% of shunt infections occur within 6 months of placement or revision. If the shunt has been in place for years without manipulation, infection is much less likely (though not impossible).[3]
The most common organism is Staphylococcus epidermidis, followed by S. aureus and gram-negatives. This is a biofilm infection on the shunt hardware — antibiotics alone are usually insufficient, and the shunt typically needs to be externalized or removed.
CSF analysis from the shunt may be negative on cell count but positive on culture. CSF must be obtained from the shunt reservoir itself, not from a lumbar puncture. A routine LP will not reliably detect shunt infection — the infection is on the hardware, not necessarily in the lumbar thecal sac.
Fever in a shunt patient is a shunt infection until proven otherwise, especially if within 6 months of surgery. Other sources (UTI, pneumonia) should be considered, but don’t let them distract you from evaluating the shunt.
The Shunt Tap
Indications: Suspected infection (CSF for cell count, gram stain, culture) or assessment of shunt function (opening pressure, ability to aspirate CSF). This is typically a neurosurgery procedure, but ED physicians should know the technique for emergent situations.
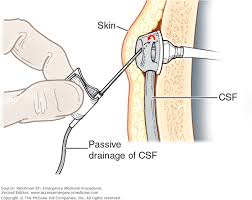
Technique: Palpate the reservoir (dome-shaped bump on the skull). Shave hair over the site. Prep with chlorhexidine or betadine. Insert a 22–23G butterfly needle at 45 degrees, angling the tip toward the center of the reservoir. Attach to manometry for opening pressure. Aspirate CSF gently — do not aspirate forcefully as this can collapse the ventricle wall onto the proximal catheter.
Opening pressure interpretation: Normal is 5–15 cm H2O. Elevated pressure suggests distal obstruction (CSF can’t drain). Very low or no flow suggests proximal obstruction (catheter not communicating with ventricles). A pressure that drops rapidly with aspiration and doesn’t refill is also concerning for proximal obstruction.
Disposition
Admit: Confirmed or suspected malfunction with symptoms, any concern for shunt infection, altered mental status, new neurologic deficits, or imaging showing acute hydrocephalus.
Discharge (with neurosurgery agreement): Mild headache in a shunt patient with reassuring imaging (stable ventricle size compared to baseline), normal neurologic exam, afebrile, able to tolerate oral intake, and reliable follow-up with neurosurgery within 24–48 hours. This should be a shared decision with the neurosurgeon — do not discharge a shunt patient with symptoms without neurosurgery input.
References
- Browd SR, Ragel BT, Gottfried ON, Kestle JR. Failure of cerebrospinal fluid shunts: part I. Obstruction and mechanical failure. Pediatr Neurol. 2006;34(2):83-92. PubMed
- Boyle TP, Nigrovic LE. Radiographic evaluation of pediatric cerebrospinal fluid shunt malfunction in the emergency setting. Pediatr Emerg Care. 2015;31(6):435-440. PubMed
- Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 IDSA clinical practice guidelines for healthcare-associated ventriculitis and meningitis. Clin Infect Dis. 2017;64(6):e34-e65. PubMed
