Last reviewed: March 2026
Contents
MDM Templates
Seizure — Simple Febrile
Child presents with generalized seizure in the setting of fever. Seizure was generalized tonic-clonic, lasted <15 minutes, and did not recur within 24 hours. Child has returned to neurologic baseline with normal mental status, normal neurologic exam, and no focal deficits.
Presentation consistent with simple febrile seizure. No features of complex febrile seizure (no focality, duration <15 minutes, single episode). Child at baseline, well appearing, tolerating oral intake. Not consistent with meningitis (no meningeal signs, at baseline), epilepsy (febrile context), or intracranial pathology (normal exam, no focal findings).[1]
Plan: Treat underlying febrile illness. Observed in ED with return to baseline. Discharge with PCP follow-up within 24 hours. Family counseled that febrile seizures do not cause brain damage and recurrence risk is approximately 30%. Return for seizure >5 minutes, focal seizure, failure to return to baseline, or signs of serious infection.
Seizure — Complex Febrile
Child presents with febrile seizure with complex features — focal onset, duration >15 minutes, or recurrence within 24 hours. Child has returned to neurologic baseline.
Complex features warrant closer evaluation. Child at baseline with normal neurologic exam, which is reassuring against ongoing intracranial process. Not consistent with meningitis or encephalitis (at baseline, no meningeal signs). Shared decision making regarding advanced workup based on clinical picture.[1]
Plan: Treat underlying febrile illness. Extended observation in ED. Disposition based on clinical trajectory and family comfort. PCP follow-up within 24 hours. Return for recurrent seizure, altered mental status, or signs of serious infection.
If not returning to baseline or concern for meningitis: LP and empiric antibiotics. CT head if focal deficits or signs of elevated ICP. Admit for monitoring and further evaluation.
Seizure — Afebrile / First-Time
Child presents with first unprovoked afebrile seizure. Has returned to neurologic baseline with normal mental status and exam. No history of prior seizures, no recent trauma, no toxic ingestion.
First unprovoked seizure in a child warrants evaluation for underlying etiology. At baseline with normal exam, which lowers concern for acute intracranial process. Differential includes epilepsy, structural lesion, metabolic derangement, and toxic ingestion. Not consistent with febrile seizure (afebrile), status epilepticus (self-limited), or acute symptomatic seizure (no identified provoking factor).[2]
Plan: Glucose and electrolytes obtained. Neurology consulted regarding need for neuroimaging and EEG. Antiepileptic medication not routinely started after a single unprovoked seizure per AAN guidelines. Discharge with neurology follow-up for outpatient EEG and MRI. Return for recurrent seizure, altered mental status, or new focal deficits.
If abnormal neurologic exam, prolonged postictal state, or concern for structural lesion: CT head in ED. MRI as outpatient or inpatient depending on findings. Admit if not at baseline or if imaging abnormal.
Seizure — Status Epilepticus
Child presenting with continuous seizure activity >5 minutes or recurrent seizures without return to baseline between episodes. This constitutes status epilepticus and requires emergent intervention to prevent neuronal injury.
Status epilepticus is a neurologic emergency. Differential for underlying etiology includes febrile status, CNS infection, metabolic derangement, toxic ingestion, structural lesion, and breakthrough seizure in known epilepsy. Refractory status (>30 minutes despite treatment) carries significant morbidity.[3]
Plan: Benzodiazepines administered per protocol. Second-line antiepileptic loaded. Glucose checked and corrected. Source of seizure investigated in parallel with seizure termination. Neurology consulted. Admit to PICU for continuous monitoring.
If refractory to benzodiazepines and second-line agent: Continuous infusion (midazolam or propofol) with intubation. Continuous EEG monitoring. Neurology and PICU involvement mandatory.
Clinical Education
Simple vs Complex Febrile Seizure
| Feature | Simple | Complex |
| Duration | <15 minutes | >15 minutes |
| Type | Generalized | Focal features |
| Recurrence in 24h | No | Yes |
| Postictal | Brief, returns to baseline | May be prolonged |
Simple febrile seizures are benign. They occur in 2-5% of children age 6 months to 5 years. They do not cause brain damage, do not increase risk of epilepsy beyond the general population (<2%), and do not require antiepileptic medication. Recurrence risk is ~30% with subsequent febrile illnesses.[1]
Antipyretics do not prevent febrile seizures. The seizure is triggered by the fever itself, not the rate of rise. Treat fever for comfort, but counsel families that antipyretics will not prevent recurrence. If the child has a known history of febrile seizures and a seizure lasts >5 minutes, families may be prescribed rectal diazepam for home use.
When to LP and When to Image
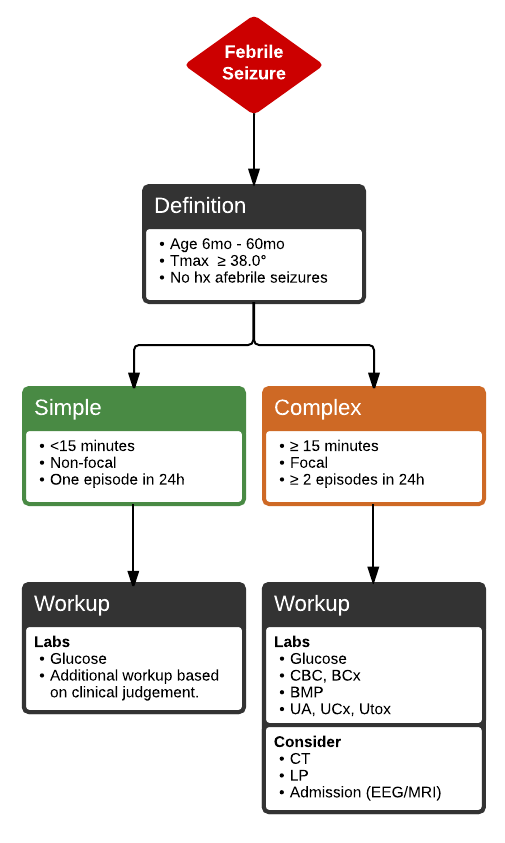
LP is NOT routine for febrile seizures. Per AAP 2011 guidelines, LP should be performed if: meningeal signs present, child not returning to baseline, child <6 months (lower threshold), or child is incompletely immunized against H. influenzae and S. pneumoniae. A child who has returned to baseline after a simple febrile seizure does not need an LP.[1]
Neuroimaging is NOT indicated for simple febrile seizures. Consider CT head for: complex febrile seizure with prolonged postictal state, focal neurologic deficit, signs of elevated ICP, or concern for trauma/NAT. For first unprovoked afebrile seizure, outpatient MRI and EEG are standard per AAN guidelines — emergent imaging only if abnormal exam.[2]
Status Epilepticus Management
Status epilepticus is defined as continuous seizure activity >5 minutes. Brain injury begins after 30 minutes of continuous seizure. The treatment ladder is time-sensitive — do not delay escalation waiting for prior agents to work.[3]
| Time | Agent | Dose |
| 0-5 min | Stabilize | ABCs, glucose, IV access |
| 5 min | Benzodiazepine (1st line) | Midazolam 0.2 mg/kg IM (max 10 mg) or lorazepam 0.1 mg/kg IV (max 4 mg) |
| 10 min | Repeat benzodiazepine | Same dose, one repeat |
| 15-20 min | 2nd line AED | Fosphenytoin 20 mg PE/kg IV or levetiracetam 60 mg/kg IV (max 4500 mg) |
| 30+ min | Refractory — continuous infusion | Midazolam gtt or propofol gtt, intubate |
IM midazolam is as effective as IV lorazepam and faster when no IV access exists — per the RAMPART trial. Do not delay treatment to establish IV access. Intranasal midazolam and rectal diazepam are alternatives.[3]
Phenobarbital (20 mg/kg IV) remains first-line for neonatal seizures. Fosphenytoin and levetiracetam are preferred second-line agents in older children. Always check glucose — hypoglycemia is the most easily reversible cause of pediatric seizures.
Neonatal Seizures
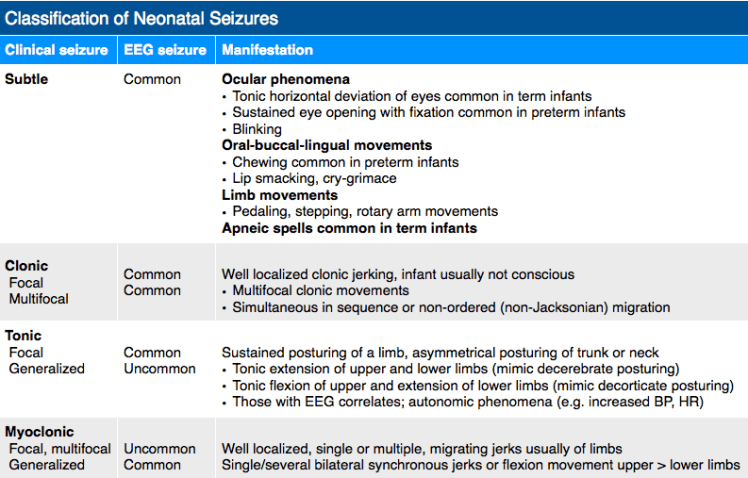
Neonatal seizures are often subtle and easy to miss. Presentations include lip smacking, tongue thrusting, eye deviation, rhythmic blinking, bicycling movements, and apnea. Tonic-clonic seizures are less common in neonates than in older children. Any repetitive stereotyped movement in a neonate should raise concern.[2]
Neonatal seizures are almost always symptomatic. Common etiologies: hypoxic-ischemic encephalopathy (most common), intracranial hemorrhage, infection (meningitis, HSV encephalitis, TORCH), metabolic (hypoglycemia, hypocalcemia, inborn errors of metabolism), and maternal drug withdrawal. Full septic workup including LP, glucose, electrolytes, and neuroimaging are indicated.
Treatment: Phenobarbital 20 mg/kg IV is first-line. Correct hypoglycemia and electrolyte abnormalities. Consider empiric acyclovir if HSV encephalitis is on the differential (maternal history, vesicular lesions, CSF pleocytosis). Neurology consultation and continuous EEG monitoring.
Infantile Spasms
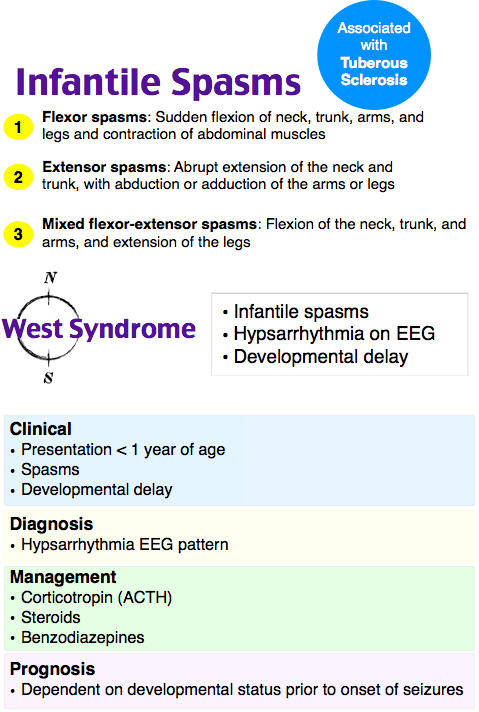
Infantile spasms (West syndrome) present as clusters of brief extensor or flexor posturing episodes, typically upon awakening. Peak onset 4-8 months. The spasms are brief (1-2 seconds) but occur in clusters of dozens. Parents often describe them as “startles” or colic. EEG shows hypsarrhythmia. This is a neurologic emergency — delayed treatment worsens developmental outcomes.[2]
If infantile spasms suspected, admit for EEG and initiation of treatment. First-line treatment is ACTH or vigabatrin (vigabatrin preferred if tuberous sclerosis). Do not dismiss clustered brief spasms in an infant as benign — normal interictal exam does not exclude the diagnosis. Neurology consultation is mandatory.
Disposition
Admit / PICU: Status epilepticus. Neonatal seizures. Infantile spasms (for EEG and treatment initiation). Not returning to baseline. Concern for meningitis or encephalitis. Abnormal neuroimaging.
Discharge: Simple febrile seizure with return to baseline and adequate observation. Complex febrile seizure at baseline with reliable follow-up. First unprovoked seizure at baseline with outpatient neurology, EEG, and MRI arranged. Return for recurrent seizure, altered mental status, focal deficits, or failure to return to baseline.
References
- Subcommittee on Febrile Seizures, AAP. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011;127(2):389-394. PubMed
- Hirtz D, Berg A, Bettis D, et al. Practice parameter: evaluating a first nonfebrile seizure in children. Neurology. 2000;55(5):616-623. PubMed
- Glauser T, Shinnar S, Gloss D, et al. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults. Epilepsy Curr. 2016;16(1):48-61. PubMed
