Last reviewed: March 2026
Contents
MDM Templates
Submersion Injury — Discharge
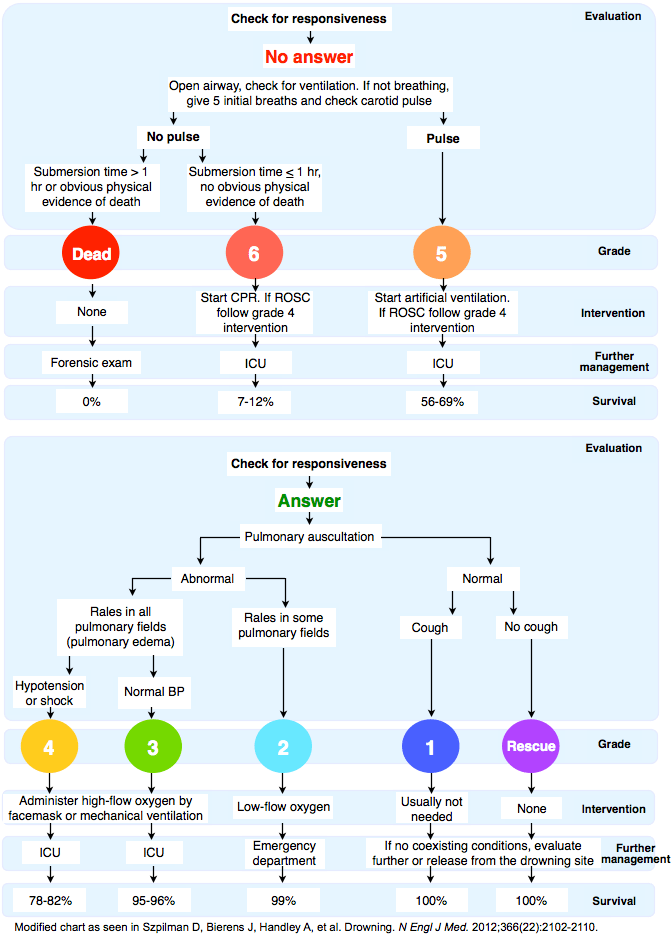
Patient presents after submersion event with no loss of consciousness, no respiratory distress, and no altered mental status. Spontaneous breathing at scene. Normal mental status on arrival. SpO2 >95% on room air.
Presentation consistent with submersion injury without significant aspiration. Normal mental status and oxygenation are the strongest predictors of good outcome. Not consistent with significant pulmonary aspiration (no hypoxia, no respiratory distress), secondary drowning pathology (no delayed respiratory decompensation after observation), or secondary precipitant requiring workup (no syncope, no seizure, no cardiac symptoms prior to event).[1]
Plan: Observation for 4-6 hours with repeat assessment. CXR if any respiratory symptoms develop. If asymptomatic with normal oxygenation at end of observation, discharge with PCP follow-up in 1-2 days. Return for cough, shortness of breath, chest pain, fever, or any respiratory symptoms.
Submersion Injury — Admit
Patient presents after submersion event with respiratory symptoms — cough, tachypnea, hypoxia, or abnormal lung sounds. May have altered mental status. Required rescue breathing or CPR at scene.
Submersion with respiratory compromise indicates significant aspiration. Aspirated water destroys surfactant, causing alveolar collapse, atelectasis, and non-cardiogenic pulmonary edema with V/Q mismatch. Hypoxia is the primary cause of morbidity and mortality. Must also consider secondary causes of submersion: intoxication, cardiac arrhythmia, seizure, or trauma (cervical spine injury from diving).[1]
Plan: Supplemental oxygen, continuous monitoring. Aggressive suctioning. Intubation with lung-protective ventilation if progressive respiratory failure. Admit for monitoring and respiratory support. ICU if intubated, persistent hypoxia, or altered mental status.
If hypothermic: Active rewarming. Maintain supine or Trendelenburg positioning to prevent cardiovascular collapse from peripheral vasodilation during rewarming.
Submersion — Cardiac Arrest
Patient in cardiac arrest after submersion event. Resuscitation initiated per ACLS with attention to the unique physiology of drowning arrest.
Drowning cardiac arrest is fundamentally a hypoxic arrest. The primary intervention is oxygenation and ventilation, not defibrillation. Presenting rhythm is typically asystole or PEA from prolonged hypoxia. Hypothermia may provide some neuroprotection, particularly in cold water submersion in pediatric patients. Cannot reliably prognosticate in the field or early in resuscitation — resuscitate aggressively until rewarmed to 32-35°C.[2]
Plan: Prioritize oxygenation — early intubation, aggressive suctioning. Standard ACLS. Rewarm to at least 32°C before terminating resuscitation (“not dead until warm and dead”). Consider ECMO if available for refractory arrest with hypothermia. Post-ROSC: targeted temperature management, ICU admission.
Clinical Education
Pathophysiology
The drowning cascade: Submersion → voluntary breath-holding → involuntary aspiration → laryngospasm → continued aspiration as laryngospasm breaks → surfactant destruction → alveolar collapse, atelectasis, non-cardiogenic pulmonary edema, V/Q mismatch → hypoxia → cardiac arrest.[1]
Fresh vs salt water distinction is clinically irrelevant. Both destroy surfactant and cause pulmonary edema. The historical teaching about electrolyte shifts from hypo/hypertonic aspiration does not apply at the volumes actually aspirated. Treat the hypoxia regardless of water type.
“Dry drowning” and “secondary drowning” are imprecise terms. The WHO recommends simply “drowning” with outcomes described as death, morbidity, or no morbidity. Delayed respiratory decompensation can occur from ongoing surfactant loss but is rare in patients who are asymptomatic after 4-6 hours of observation.[1]
Secondary Causes
Always consider why the patient drowned. Submersion may be the symptom, not the disease. Alcohol and drug intoxication are the most common precipitants in adults. Also consider: cardiac arrhythmia (long QT, Brugada, WPW), seizure, hypoglycemia, syncope, stroke, and trauma (cervical spine injury from diving).[1]
In children, non-accidental trauma must be considered when the history is inconsistent with the child’s developmental stage, there is a delay in seeking care, or the mechanism does not match the clinical findings.
Cervical spine injury: Maintain spinal precautions in any submersion event involving diving, surfing, water slides, or unknown mechanism. Alcohol intoxication impairs the ability to report neck pain.
Cold Water Submersion
Cold water submersion has a distinct physiology. The cold shock response occurs in the first minute — gasping, hyperventilation, and tachycardia that can trigger aspiration and arrhythmia. Cold incapacitation occurs at 1-10 minutes — loss of extremity function leading to inability to swim. Severe hypothermia develops at 30-60 minutes.[2]
Hypothermia may be neuroprotective, especially in children. Rapid core cooling before cardiac arrest provides some degree of brain protection. Intact neurologic survival has been reported after prolonged submersion (up to 60+ minutes) in very cold water, particularly in pediatric patients.
Rewarming considerations: Keep the patient supine or in Trendelenburg — upright positioning can cause cardiovascular collapse as peripheral vasodilation from rewarming redistributes blood volume. Patients lose their catecholamine surge once rescued, so vasopressors may be needed. Be aware that hypothermic patients are highly arrhythmogenic.
Resuscitation Pearls
Drowning arrest is a hypoxic arrest — prioritize ventilation. Unlike typical cardiac arrest where compressions come first (C-A-B), drowning resuscitation may benefit from early rescue breaths (A-B-C approach). Early intubation and aggressive suctioning of aspirated water are critical.[2]
Do not perform abdominal thrusts (Heimlich) to remove water. This does not clear aspirated water from the lungs and risks aspiration of gastric contents. Decompress the stomach with an OG/NG tube after intubation — the stomach will be full of swallowed water, and gastric distension impairs ventilation.
Prophylactic antibiotics are not indicated. Aspiration pneumonia from drowning is a chemical/inflammatory process, not infectious. Antibiotics only if clinical signs of infection develop. Similarly, bronchodilators (albuterol) are not routinely helpful — the pathology is surfactant loss and alveolar flooding, not bronchospasm.
Termination of resuscitation: If the patient remains in asystole after rewarming to at least 32°C and >20 minutes of ACLS, termination may be considered. Do not terminate in hypothermic patients who have not been rewarmed.[2]
Disposition
Discharge: Asymptomatic after 4-6 hours of observation. Normal SpO2 on room air. Normal mental status. Normal CXR (if obtained). No concerning secondary cause identified. PCP follow-up in 1-2 days. Return for any respiratory symptoms, cough, chest pain, or fever.
Admit (floor/telemetry): Any persistent respiratory symptoms. Hypoxia requiring supplemental oxygen. Abnormal CXR. Concern for secondary cause requiring workup (arrhythmia, seizure). Need for serial neurologic exams.
Admit (ICU): Intubated. Persistent hypoxia despite supplemental oxygen. Altered mental status. Post-cardiac arrest (ROSC). Hypothermia requiring active rewarming.
