Last reviewed: March 2026Contents
MDM Templates
Asymptomatic Hypertension
Patient presents to the emergency department with elevated blood pressure.
Patient is otherwise asymptomatic without confusion, chest pain, hematuria, visual changes, or SOB.
No evidence of end-organ damage.
No evidence to suggest ACS, heart failure, renal failure, stroke, or hypertensive encephalopathy.
Disposition: Discussed with patient their elevated blood pressure and need for close outpatient management of their hypertension.
Rx: Will provide a prescription for *** and instruct the patient to follow up in a primary care clinic within 1 week. Return for headache, chest pain, vision changes, confusion, or shortness of breath.
Refractory Hypertension
Patient presents with symptomatic and significantly elevated blood pressure.
They required IV antihypertensives in the ED to achieve adequate BP control.
No evidence of acute end-organ damage on workup.
Workup: CBC, BMP, UA, troponin, ECG
Findings: No evidence of AKI, troponin negative, ECG without ischemic changes, no hematuria.
Interventions:
- IV antihypertensives administered
- Pain/anxiety addressed
- Serial BP monitoring
Despite achieving transient BP reduction with IV agents, patient’s hypertension is refractory and requires a more aggressive regimen than can be safely initiated and titrated in the ED setting. Transient response to IV push medications does not equate to sustained outpatient control.
Disposition: Admit for continued BP monitoring, initiation/optimization of an oral antihypertensive regimen, and medicine consultation to establish a sustainable outpatient plan prior to discharge.
Hypertensive Emergency
Patient presented with severely elevated blood pressure with evidence of acute end-organ damage effects.
Emergent differential included hypertensive encephalopathy, intracranial hemorrhage, ACS, aortic dissection, acute heart failure/pulmonary edema, eclampsia, acute renal failure.
Interventions:
- Arterial line placement for continuous BP monitoring
- IV antihypertensive: *** (see agent selection below)
- Target: 20-25% MAP reduction in first hour (except aortic dissection and ICH — see specific targets)
Disposition: Admit to ICU for continuous monitoring and IV antihypertensive titration.
Clinical Education
Asymptomatic vs Refractory vs Emergency
Asymptomatic hypertension: Elevated BP without symptoms or end-organ damage. Start or restart oral meds, arrange PCP follow-up within 1 week. Do not aggressively lower in the ED — risks hypoperfusion injury with no benefit.[1]
Refractory hypertension: Severely elevated BP requiring IV agents in the ED to achieve any meaningful reduction. Even without end-organ damage, if a patient needs IV hydralazine or nicardipine to get their BP down, sending them home with an amlodipine script is not adequate. These patients need admission for monitored initiation of an aggressive oral regimen — getting the BP down with a one-time IV push does not mean it will stay down. They need sustained control before discharge.[1]
Hypertensive emergency: Severely elevated BP WITH acute end-organ damage — encephalopathy, ICH, ACS, aortic dissection, acute pulmonary edema, eclampsia, AKI, retinal hemorrhages/papilledema. This requires IV antihypertensive drips and ICU admission.[1]
The number doesn’t define the emergency — the end-organ damage does. A patient with a BP of 210/120 and a headache who has a normal neuro exam, normal creatinine, negative troponin, and no papilledema does not have a hypertensive emergency. But if they needed IV meds to get below 180, they shouldn’t go home on a single oral agent and a prayer.
Don’t forget pain and anxiety: Treat the pain first, recheck BP. Fentanyl is a good option — short-acting and lacks the histamine release of morphine. Many elevated BPs in the ED resolve with analgesia and anxiolysis alone.
End-Organ Damage Workup
| Target Organ | Findings | Workup |
| Brain | Encephalopathy, seizure, focal deficits, ICH | CT head, neuro exam |
| Heart | ACS, acute pulmonary edema, aortic dissection | ECG, troponin, BNP, CXR |
| Kidney | Acute kidney injury, hematuria | BMP (Cr), UA |
| Eyes | Papilledema, retinal hemorrhages, exudates | Fundoscopic exam |
| Vascular | Aortic dissection | CTA chest/abd, BP differential between arms |
| Heme | MAHA (schistocytes, thrombocytopenia) | CBC, peripheral smear, LDH, haptoglobin |
IV Antihypertensive Agents
| Agent | Mechanism | Dosing | Pearls |
| Nicardipine | Arterial vasodilation, no HR effect | Start 5mg/hr, titrate up by 2.5mg/hr q5-15min. Once at goal: decrease to 3mg/hr and re-titrate to avoid overshoot hypotension. | Most predictable and titratable. First-line for most hypertensive emergencies.[2] |
| Labetalol | Alpha + beta blockade (vasodilation, negative inotropy, mild chronotropy) | 10-20mg IV push, double dose q10min (20→40→80mg). Max 300mg. Or drip 0.5-2mg/min. | Long duration — hard to titrate. Rarely has dramatic BP effect. Safe in pregnancy. Avoid in acute HF, bradycardia, asthma.[2] |
| Esmolol | Beta-1 selective | Bolus 0.5mg/kg over 1min, drip 0.05mg/kg/min, titrate to goal. If no effect → re-bolus and increase drip. | Primarily reduces HR. Ultra-short half-life (9min) — very titratable. Good for aortic dissection (HR control).[3] |
| Nitroglycerin | Venodilation > arterial dilation | Start 5-10mcg/min, titrate by 5-10mcg q3-5min. | Best for ACS and acute pulmonary edema. Turns off immediately when stopped. Avoid with PDE-5 inhibitors.[2] |
| Clevidipine | Arterial vasodilation (dihydropyridine CCB) | Start 1-2mg/hr, double q90sec initially, then titrate by smaller increments. | Ultra-short half-life (1min). Very titratable. Lipid emulsion — avoid in soy/egg allergy. Expensive.[4] |
AVOID: Nitroprusside (cyanide toxicity, very labile) and Hydralazine (unpredictable magnitude/duration of effect, reflex tachycardia) — both are poor choices in the ED despite historical use.[2]
Oral Agents for ED Discharge
2025 AHA/ACC guideline update: For stage 2 hypertension (≥140/90), guidelines now recommend initiating dual therapy with two first-line agents of different classes, preferably as a single-pill combination (SPC) to improve adherence and reduce time to BP control.[5]
Preferred initial combinations:
- ACEi or ARB + CCB (e.g., Amlodipine/Benazepril)
- ACEi or ARB + thiazide diuretic (e.g., Lisinopril/HCTZ, Losartan/HCTZ)
| Agent | Dose | Notes |
| Amlodipine | 5-10mg PO daily | CCB. No labs needed. Takes days to reach full effect. Good combo partner with ACEi/ARB. |
| Lisinopril | 10-20mg PO daily | ACEi. Preferred with CKD or diabetes (renoprotective). Check Cr/K+ at follow-up. Avoid in pregnancy. |
| Losartan | 50-100mg PO daily | ARB alternative to ACEi (if ACEi cough). Same CKD/DM benefit. Avoid in pregnancy. |
| HCTZ | 12.5-25mg PO daily | Thiazide. Common combo partner. Check BMP at follow-up (hypokalemia, hyponatremia). Chlorthalidone 12.5-25mg is a more potent alternative. |
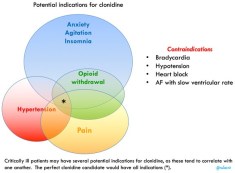
| Clonidine | 0.1-0.2mg PO | Alpha-2 agonist. Good for combined HTN + pain + anxiety. Onset 30min, peak 60-90min. Modest drop ~20/10. Tachyphylaxis develops quickly — poor long-term monotherapy. NOT a first-line agent.[6] |
Stage 1 hypertension (130-139/80-89): Single agent is still appropriate. Monotherapy with any first-line class (ACEi, ARB, CCB, or thiazide).[5]
Key principle: The ED is not the place to normalize blood pressure in asymptomatic patients. Start meds, arrange follow-up within 1 week, and let the outpatient provider titrate. Acute lowering of chronic hypertension risks watershed stroke and myocardial ischemia.[1]
Outpatient Lab Follow-Up by Agent
What the PCP needs to check:
| Agent | Labs needed at follow-up | What you’re watching for |
| ACEi / ARB | BMP at 1-2 weeks | Cr rise (>30% = stop), hyperkalemia |
| HCTZ / Chlorthalidone | BMP at 1-2 weeks | Hypokalemia, hyponatremia, Cr rise, hyperglycemia |
| ACEi/ARB + Thiazide combo | BMP at 1-2 weeks | K+ may balance out (ACEi raises, thiazide lowers) but still check. Cr rise. |
| ACEi/ARB + CCB combo | BMP at 1-2 weeks | Cr rise, hyperkalemia (from the ACEi/ARB component). CCB itself needs no labs. |
| CCB alone (Amlodipine) | None required | No metabolic effects. Peripheral edema is main side effect. |
Why ED docs hesitate on thiazides — and why they shouldn’t: The concern is prescribing HCTZ from the ED without lab follow-up. But BMP at 1-2 weeks is all that’s needed, and that’s the PCP’s job at the follow-up visit you’re already arranging. The risk of sending a patient home with uncontrolled hypertension and no medication is greater than the risk of hypokalemia at 2 weeks. If you’re still uncomfortable, the ACEi/ARB + CCB combo (e.g., Amlodipine/Benazepril) avoids the electrolyte issue entirely — the CCB component requires no lab monitoring, and the ACEi/ARB just needs a Cr/K+ check at follow-up.[5]
Practical tip: When discharging, document: “Patient prescribed [combo]. Labs (BMP) to be checked by PCP at 1-2 week follow-up to assess renal function and electrolytes.” This makes the handoff explicit and protects you.
Specific Hypertensive Emergencies
Aortic dissection: Most aggressive target. Goal HR <60 AND SBP <120 within 20 minutes. Start esmolol (rate control first), then add nicardipine if SBP still elevated. Beta-blockade BEFORE vasodilation — vasodilators alone cause reflex tachycardia which increases aortic shear stress.[3]
Intracranial hemorrhage: AHA guidelines recommend SBP <140 if presenting SBP 150-220 (INTERACT2, ATACH-2 trials).[7] Nicardipine or clevidipine drip preferred. Avoid aggressive lowering below 130 (ATACH-2 showed increased renal AEs without benefit).
Acute ischemic stroke: Do NOT lower BP unless >220/120, or >185/110 if tPA candidate. Permissive hypertension maintains cerebral perfusion to the penumbra.[8]
Acute pulmonary edema: Nitroglycerin drip is first-line (venodilation reduces preload). High-dose NTG boluses (400-800mcg) can be used for rapid effect while drip is being set up. Add BiPAP. Avoid beta-blockers in acute decompensated HF.[2]
Eclampsia/severe preeclampsia: Magnesium sulfate 4-6g IV bolus then 1-2g/hr drip for seizure prophylaxis/treatment. For BP: Labetalol IV (safe in pregnancy) or Hydralazine 5-10mg IV q20min (one scenario where hydralazine is still used). Nicardipine is also safe. Target SBP <160, DBP <110. Avoid ACEi/ARBs, nitroprusside.[9]
Sympathomimetic crisis (cocaine, amphetamines): Benzodiazepines first-line (treats the underlying sympathetic surge). Add nitroglycerin or nicardipine if BP still elevated. Traditional teaching says avoid beta-blockers (unopposed alpha stimulation) — though recent evidence suggests labetalol is probably safe, most toxicologists still prefer the benzo + vasodilator approach.[10]
References
- 2025 AHA/ACC Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults. Circulation. 2025. AHA Journals
- Varon J, Marik PE. Clinical Review: The Management of Hypertensive Crises. Crit Care. 2003;7(5):374-384. PubMed
- Hiratzka LF et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease. Circulation. 2010;121(13):e266-e369. PubMed
- Pollack CV et al. Clevidipine for Acute Hypertension: Results of the VELOCITY Trial. Anesth Analg. 2009;108(4):1052-1059. PubMed
- 2025 AHA/ACC Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults. Circulation. 2025. AHA Journals — See also: JournalFeed Summary
- Elghozi JL et al. Clonidine Reduces Blood Pressure and Heart Rate in Hypertensive Patients. Eur J Clin Pharmacol. 1991;41(1):59-63. PubMed
- Anderson CS et al. Rapid Blood-Pressure Lowering in Patients with Acute Intracerebral Hemorrhage (INTERACT2). N Engl J Med. 2013;368(25):2355-2365. PubMed
- Powers WJ et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update. Stroke. 2019;50(12):e344-e418. PubMed
- ACOG Practice Bulletin No. 222: Gestational Hypertension and Preeclampsia. Obstet Gynecol. 2020;135(6):e237-e260. PubMed
- Richards JR et al. Treatment of Cocaine Cardiovascular Toxicity: A Systematic Review. Clin Toxicol. 2016;54(5):345-364. PubMed
