Last reviewed: March 2026Contents
MDM Templates
Dental Pain / Caries
Patient with dental pain localized to tooth #***.
They do NOT have high-risk features such as immunosuppression or fever.
They are nontoxic appearing, with stable vitals, no trismus, no floor-of-mouth swelling, and no dysphagia or voice change.
Exam without periapical swelling, fluctuance, or pus expression.
No tooth fracture or mobility.
History and exam lower suspicion for periapical abscess, Ludwig’s angina, PTA, RPA, and other significant odontogenic infections.
Plan: Ibuprofen 600mg PO q6h.[1] Defer antibiotics for dental pain alone without evidence of infection.[2]
Disposition: Discharge with dental follow-up within 48-72 hours. Return precautions for fever, facial swelling, difficulty swallowing or breathing.
Dental Abscess
Patient with dental pain and localized facial/periapical swelling consistent with dental abscess.
They do NOT have high-risk features such as immunosuppression or fever.
They are nontoxic appearing, with stable vitals, no trismus, no floor-of-mouth swelling, and no dysphagia or voice change.
History and exam lower suspicion for deep space/severe oropharyngeal infections (Ludwig’s angina, PTA, RPA) and other airway-threatening processes.
Drainable abscess:
I&D performed — incision at most fluctuant point, blunt dissection, expression of purulence, NS irrigation.
Plan: Amoxicillin 500mg PO TID x 7d (Clindamycin 300mg TID if PCN allergy). Ibuprofen + acetaminophen.
Disposition: Discharge with dental follow-up within 24-48 hours.
Cellulitis without drainable collection:
Plan: Augmentin 875mg PO BID x 7d (Clindamycin 300mg TID if PCN allergy). Ibuprofen + acetaminophen.
Disposition: Discharge with close dental follow-up.
Admit if: Trismus (<2cm opening), floor-of-mouth swelling, toxic appearance, immunosuppression, failed outpatient therapy, or concern for deep space infection. CT neck with IV contrast. Unasyn 3g IV q6h. ENT/OMFS consult.
Dental Trauma
Patient with dental injury after trauma to tooth/teeth #___. Midface stable. No malocclusion. No mandible step-off or point tenderness along body, angle, or condyle. Sublingual space without brawny edema or tongue elevation.
Subluxation/Luxation:
Dental block performed. Tooth repositioned and splinted with Coe-Pak/Dermabond bridge to adjacent teeth.
Plan: Soft diet x 2 weeks. Ibuprofen. Chlorhexidine rinse BID.
Disposition: Discharge with dental follow-up within 24 hours.
Avulsion — permanent tooth:
Tooth stored in ___ (Hanks/milk/saliva). Reimplanted within ___ minutes and splinted in place.
Plan: Doxycycline 100mg BID x 7d. Soft diet. Chlorhexidine. Tetanus updated.
Disposition: Discharge with emergent dental follow-up within 24 hours.[3]
Primary tooth avulsion: Do NOT reimplant — risk of damage to permanent tooth bud. Dental follow-up for space maintenance.[3]
Ellis fracture — see classification below.
Post-Extraction Bleeding
Patient with bleeding from extraction site ___ hours/days post-extraction. No active anticoagulation / on ___. No signs of infection. Hemodynamically stable.
Interventions: Direct pressure with dampened gauze x 30 min. If persistent — topical TXA-soaked gauze, Surgicel/Gelfoam packing, or figure-of-eight absorbable suture across socket.
Plan: Avoid spitting, straws, smoking x 48h. Soft diet.
Disposition: Discharge with dental follow-up. Return for rebleeding.
Clinical Education
Pain Management
Ibuprofen 400-600mg + acetaminophen 1000mg is superior to opioids for dental pain. NNT for ibuprofen alone is 2.5 — one of the best analgesic-to-indication matches in EM.[1] Antibiotics do not treat pain and should not be prescribed for dental caries without evidence of infection.[2]
Dry socket (alveolar osteitis): Pain 2-5 days post-extraction, empty socket without clot. Not an infection — no antibiotics. Irrigate, pack with eugenol gauze or dry socket paste, ibuprofen, dental follow-up 24 hours.[6]
Ellis Classification
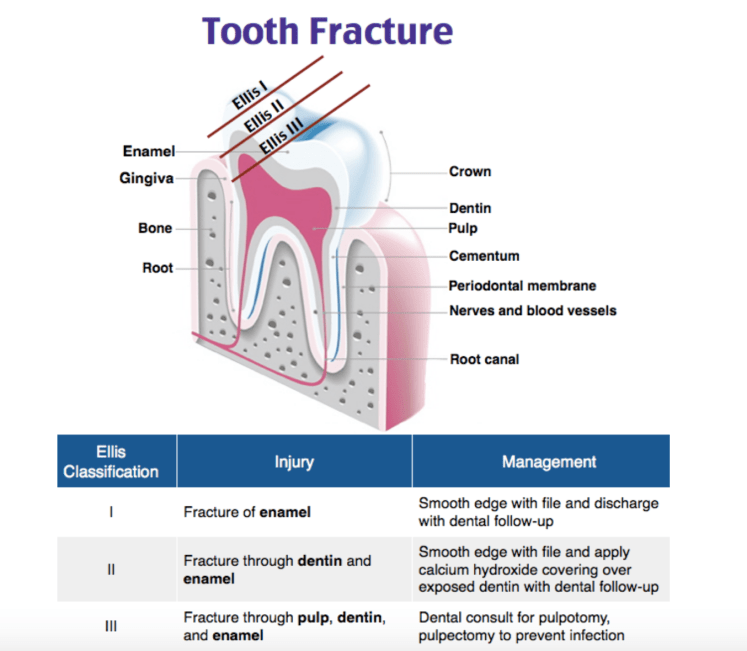
| Class | Structure | Appearance | Management |
| I | Enamel only | White, rough edge | Smooth edges, routine dental f/u |
| II | Enamel + dentin | Yellow layer, temp sensitive | CaOH paste (Dycal), dental f/u 24h[4] |
| III | Enamel + dentin + pulp | Pink/bleeding center | CaOH paste, emergent dental/OMFS[4] |
Alveolar fractures (bone segment moves with the teeth) require CT and OMFS. Always palpate full mandibular body, angle, and condyles — panorex if any concern.[4]
Avulsed Tooth
Reimplantation success drops significantly after 60 minutes — best within 5 minutes. Storage media best to worst: Hanks Balanced Salt Solution (Save-A-Tooth) > cold milk > buccal vestibule (saliva) > saline > water. Never scrub the root.[3]
Technique: irrigate socket, remove clot, reinsert with gentle digital pressure, splint to adjacent teeth. Rx doxycycline (amoxicillin if <12y). Tetanus if not current. Do NOT reimplant primary teeth.[3]
Dental Nerve Blocks
IANB (mandibular teeth): Landmark is pterygomandibular raphe. Needle ~1cm above occlusal plane of lower molars, lateral to raphe. Advance to bone, withdraw 1mm, aspirate, inject 1.5-2mL lido w/ epi. Blocks all ipsilateral mandibular teeth + lower lip + chin. Add a long buccal block (~1mL in buccal mucosa distal to last molar) for molar procedures — IANB alone misses buccal gingiva.[7]
Maxillary teeth: Simple supraperiosteal infiltration — 1-2mL lido w/ epi into buccal vestibule at apex of target tooth. Maxillary bone is thin enough for direct infiltration to work reliably.[7]
Pearl: Blocks often fail in active infection (acidic pH reduces local anesthetic efficacy). Use higher-volume blocks or consider procedural sedation for large abscess I&D.
Antibiotic Selection
| Indication | First-Line | PCN Allergy |
| Periapical abscess (after I&D) | Amoxicillin 500mg TID x 7d | Clindamycin 300mg TID x 7d |
| Facial cellulitis | Augmentin 875mg BID x 7d | Clindamycin 300mg TID x 7d |
| ANUG | Amoxicillin 500mg TID + Flagyl 500mg TID x 7d | Clindamycin 300mg TID x 7d |
| Deep space infection (admit) | Unasyn 3g IV q6h | Clindamycin 900mg IV q8h |
Dental infections are polymicrobial (oral strep + anaerobes). Clindamycin is the universal PCN-allergy alternative — covers both.[2]
ANUG
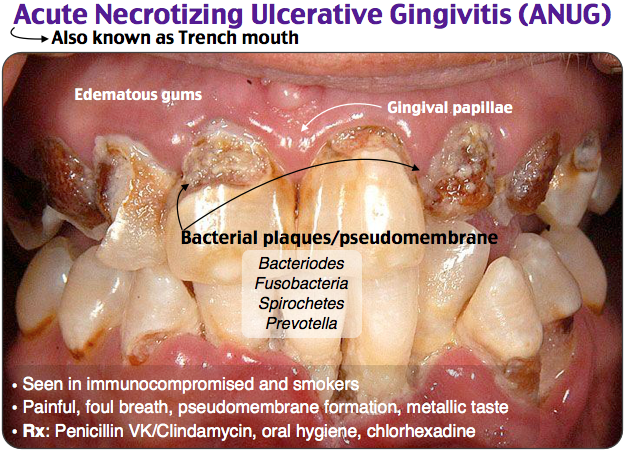
Classic triad: pain, ulcerated/”punched out” interdental papillae, fetor oris. Think young adults with poor hygiene, stress, or immunosuppression. Consider HIV testing if recurrent or severe.[8] Treat with amoxicillin + metronidazole (or clindamycin), chlorhexidine rinse BID, dental follow-up 48h for debridement.
Ludwig’s Angina
Bilateral submandibular/sublingual/submental space infection, usually from mandibular molar source. Classic: “woody” floor of mouth, tongue elevation, drooling, muffled voice. This is an airway emergency first — prepare for difficult airway (fiberoptic, surgical backup). CT neck with IV contrast. Unasyn 3g IV q6h. Dexamethasone 10mg IV. Emergent ENT/OMFS for operative drainage. Do not lay supine if in respiratory distress.[5] See also: Radiopaedia: Ludwig’s Angina.
References
- Moore PA et al. Benefits and Harms Associated with Analgesic Medications Used in the Management of Acute Dental Pain. JADA. 2018;149(4):256-268. PubMed
- ADA Clinical Practice Guidelines. Antibiotic Use for Emergency Management of Symptomatic Irreversible Pulpitis. JADA. 2019;150(12):e193. PubMed
- Fouad AF et al. IADT Guidelines: Avulsion of Permanent Teeth. Dent Traumatol. 2020;36(4):331-342. PubMed
- Bourguignon C et al. IADT Guidelines: Crown Fractures and Luxation Injuries. Dent Traumatol. 2020;36(4):314-330. PubMed
- Boscolo-Rizzo P, Da Mosto MC. Submandibular Space Infection: A Potentially Lethal Infection. Int J Infect Dis. 2009;13(3):327-333. PubMed
- Kolokythas A et al. Alveolar Osteitis: A Comprehensive Review. Int J Dent. 2010;2010:249073. PubMed
- Benko K. Emergency Dental Procedures. Roberts and Hedges’ Clinical Procedures in Emergency Medicine. 7th ed. 2019.
- Herrera D et al. Acute Periodontal Lesions. J Clin Periodontol. 2018;45(Suppl 20):S78-S94. PubMed

I use your dot phrases on a daily basis! I love them. I work for Kaiser, so we use Epic and it has saved me so much time having these. Thank you! I feel like I owe you a million dollars, or at least a Starbucks!
LikeLike
Thanks Heather! Glad it could help
LikeLike
A long time late reply as I haven’t been on here much since residency, but ready for a reboot with the new documentation guidelines; appreciate the support!
LikeLike