Last reviewed: March 2026
Contents
MDM Templates
Knee Sprain
Patient presents with knee pain after injury. They deny mechanical locking, instability with ambulation, and inability to bear weight. They are well appearing with a stable joint on exam, intact neurovascular status, and soft compartments.
Presentation most consistent with knee sprain without joint instability. History, exam, and workup not consistent with fracture, dislocation, compartment syndrome, or neurovascular injury.
Plan: RICE protocol and analgesics.
Disposition: Discharge with return precautions for worsening pain, inability to bear weight, mechanical locking, or new swelling. Follow up with PCP within 1 week.
Patellar Dislocation
Patient presents with lateral patellar dislocation of their *** knee, successfully reduced at bedside. They are neurovascularly intact distally with soft compartments.
History and exam not consistent with fracture, compartment syndrome, or neurovascular injury. The dislocation has been satisfactorily reduced and immobilized, and the patient has been given appropriate analgesia.
Plan: Knee immobilizer in extension. Analgesics.
Disposition: Discharge with return precautions and orthopedic follow-up within 1 week.
Knee / Tibial Plateau Fracture
Patient presents with knee pain and inability to bear weight after injury. Imaging demonstrates fracture. They do not currently demonstrate complications such as compartment syndrome, neurovascular injury, or open fracture.
If non-displaced / low-energy: Fracture has been immobilized in a knee immobilizer. The patient is made non-weight-bearing on the affected extremity with crutches.
Plan: Analgesics. Orthopedic follow-up within 1 week.
Disposition: Discharge.
If displaced, comminuted, or high-energy mechanism:
Orthopedics consulted regarding fracture pattern, need for operative fixation, and admission.
Procedure Notes
Knee Arthrocentesis
Location: *** knee, *** approach
Time Out: Correct patient, correct procedure confirmed
Consent: Obtained with appropriate read back of understanding
Anesthesia: Local anesthesia with 1% lidocaine
Approach: Knee placed at approximately 15 degrees of flexion. The entry point was prepped and cleansed in sterile fashion. An 18-gauge needle was inserted into the knee joint under direct palpation guidance.
Findings: *** mL of *** fluid aspirated. Sent for cell count, crystal analysis, gram stain, and culture.
Injection: *** mL of 1% lidocaine mixed with *** mg triamcinolone injected through the same access site
Complications: None. Patient tolerated procedure well.
Clinical Education
Ottawa Knee Rules
The Ottawa Knee Rules have ~99% sensitivity for fracture and can safely reduce imaging by 30–40%. Image the knee if any of the following are present: age ≥55, isolated patellar tenderness, tenderness at the fibular head, inability to flex the knee to 90 degrees, or inability to take 4 weight-bearing steps in the ED.[1]
The rules do not apply to patients under 18, and do not reliably detect ligamentous injuries, meniscal tears, or patellar dislocations — those are clinical diagnoses that may need MRI as an outpatient.
X-Ray Pearls — Ligamentous Injury on Plain Film
A Segond fracture is pathognomonic for ACL tear. This is a small avulsion fragment off the lateral tibial plateau — look for it on the AP view. If you see it, the patient has an ACL tear until proven otherwise, even if the knee feels stable on exam.[2]
PCL avulsion fractures appear as a bone fragment off the posterior tibial plateau — classic dashboard injury mechanism (knee strikes dashboard with posterior tibial force). ACL avulsion fractures (tibial eminence/spine fractures) are more common in adolescents and occur with hyperextension mechanisms.
Don’t mistake a fabella for a fracture. A fabella is a normal accessory ossicle in the lateral gastrocnemius tendon — it’s round, corticated, and sits posterior to the lateral femoral condyle. A Segond fragment is irregular, has sharp edges, and sits just off the lateral tibial plateau margin.
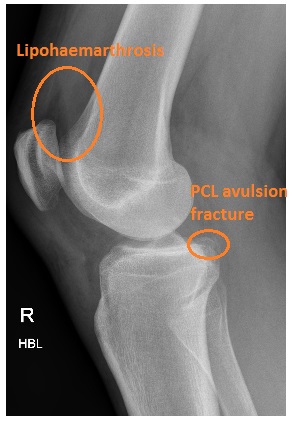
PCL Avulsion Fracture

Segond Fracture

Fabella (red circle) — normal accessory ossicle, can mimic Segond fracture
Traumatic Knee Effusion
A tense traumatic effusion usually contains blood (hemarthrosis). If you aspirate a traumatic knee effusion and get frank blood, think ACL tear (~70% of traumatic hemarthroses), tibial plateau fracture, or patellar dislocation with osteochondral fragment. If fat globules float on top of the blood (lipohemarthrosis), there is an intra-articular fracture — it may be occult on plain films and need CT.[3]
Patellar Dislocation Pearls
Most patellar dislocations are lateral and reduce spontaneously or with knee extension. Reduction technique: extend the knee while gently pushing the patella medially. Most reduce easily. Post-reduction, immobilize in a knee immobilizer (full extension) and make them non-weight-bearing initially.[4]
Get a post-reduction X-ray. You’re looking for osteochondral loose bodies — the medial patellar facet can shear off a fragment during dislocation. If you see a loose body, orthopedics needs to know, as it may need arthroscopic removal. First-time dislocators with osteochondral fractures have higher rates of surgical intervention.
Tibial Plateau Fracture Pearls
Tibial plateau fractures are high-energy injuries with a high complication rate. Always assess for compartment syndrome (the most feared complication), popliteal artery injury, and peroneal nerve injury (check dorsiflexion and lateral leg sensation). The Schatzker classification guides management — types I–III are often non-operative, types IV–VI typically need surgery.[5]
CT is almost always needed. Plain films underestimate the degree of articular depression and comminution. If you see a tibial plateau fracture on X-ray, get a CT before calling ortho — they’ll want it to plan management.
Septic Joint Considerations
If you’re tapping a hot, swollen knee, always send fluid for cell count, crystal analysis, gram stain, and culture. WBC >50,000 on synovial fluid is the classic septic threshold, but gout can exceed this. The combination of synovial WBC >50,000, inability to bear weight, fever, and ESR >30 increases probability significantly — but no single finding rules it in or out. If suspicion is high, treat empirically and admit.[6]
References
- Stiell IG et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA. 1996;275(8):611-615. PubMed
- Gottsegen CJ et al. Avulsion fractures of the knee: imaging findings and clinical significance. RadioGraphics. 2008;28(6):1755-1770. PubMed
- Lee JH et al. Lipohemarthrosis of the knee: a review of recent experiences. Korean J Radiol. 2001;2(3):163-166. PubMed
- Gravesen KS et al. Treatment of acute patellar dislocation: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):831-844. PubMed
- Prat-Fabregat S, Camacho-Carrasco P. Treatment strategy for tibial plateau fractures: an update. EFORT Open Rev. 2016;1(5):225-232. PubMed
- Margaretten ME et al. Does this adult patient have septic arthritis? JAMA. 2007;297(13):1478-1488. PubMed
