Last reviewed: March 2026Contents
MDM Templates
Simple Laceration
Patient with a *** cm laceration to the *** sustained by ***.
Wound explored down to a clear and bloodless field — no evidence of retained foreign body or injury to underlying structures. Neurovascular status intact. No surrounding erythema, warmth, or signs of infection. Tetanus UTD / updated today.
History and exam lower suspicion for involvement of deeper structures including bone, tendon, nerve, major vessel.
Wound irrigated with high-volume NS and closed with *** sutures in simple interrupted fashion. Patient tolerated procedure well.
Plan: Wound care instructions, keep dry x 24h then gentle cleansing daily. Defer antibiotics given clean wound, location, and timing.
Disposition: Discharge with PCP/wound recheck in 2 days. Suture removal in 7 days. Return precautions for signs of infection.
Facial Laceration
Patient with a *** cm laceration to the face/*** sustained by ***.
Wound explored — no retained foreign body.
No underlying facial fracture on exam.
Facial nerve function intact (forehead raise, eye closure, smile symmetric).
Parotid duct intact (no clear fluid from Stensen’s duct).
No involvement of the lip vermilion border / eyelid margin / ear cartilage / nasal cartilage.
History and exam lower suspicion for facial fracture, facial nerve injury, parotid duct injury, and lacrimal duct injury.
Procedure summary: Wound irrigated and closed with *** sutures with meticulous attention to cosmesis and tissue edge eversion. Deep layer closed with *** absorbable sutures where applicable.
Plan: Keep clean, petroleum jelly to wound, sun protection x 6-12 months to minimize scar.[1]
Disposition: Discharge. Suture removal in 4-5 days. PCP or plastics follow-up if cosmetic concern.
Scalp Laceration
Patient with a *** cm scalp laceration sustained by ***.
Wound explored, no galea violation noted.
No palpable skull fracture or bony step-off. No signs of intracranial injury on exam.
Tetanus UTD.
History and exam lower suspicion for skull fracture, intracranial hemorrhage, and retained foreign body.
Wound irrigated and closed with staples. Hemostasis achieved.
Plan: Wound care, may wash hair gently after 24 hours.
Disposition: Discharge. Staple removal in 7-10 days. Return precautions for head injury and wound infection signs.
Tongue / Intraoral Laceration
Patient with a *** cm laceration to the tongue / buccal mucosa / lip sustained by ***.
No active hemorrhage.
Wound does not involve the tongue margin, is not gaping, and does not bisect the tongue.
No dental injury.
No floor-of-mouth swelling.
Small, non-gaping, not on tongue margin:
Plan: No repair needed — oral mucosa heals rapidly. Chlorhexidine rinse BID. Soft diet x 5 days.
Disposition: Discharge with dental/PCP follow-up PRN.
Gaping, on tongue margin, or through-and-through:
Anesthesia: Topical 4% lidocaine gauze followed by local infiltration. Wound irrigated with NS. Closure with 4-0 or 5-0 absorbable suture (Vicryl/chromic gut) in loose, full-thickness interrupted fashion.[2]
Plan: Chlorhexidine rinse BID. Soft diet. No antibiotics for clean intraoral wounds.
Disposition: Discharge. Sutures will dissolve. Return for bleeding, swelling, or signs of infection.
Procedure Notes
Suture Repair
Location: *** cm *** laceration to the ***
Time Out: Correct patient, correct procedure confirmed
Anesthesia: Local infiltration with *** / topical LET / digital block
Approach: Wound prepped and cleansed in usual fashion. Copiously irrigated with normal saline under high pressure.
Exploration: Wound explored in a clear and bloodless field to the base. No evidence of foreign body or injury to underlying structures.
Methods: Deep layer closed with *** absorbable sutures / no deep layer needed. Skin closed with *** sutures in simple interrupted / running fashion. Wound edges well-apposed with good eversion. Hemostasis achieved.
Complications: None. Patient tolerated procedure well.
Staple Repair
Location: *** cm *** laceration to the scalp
Time Out: Correct patient, correct procedure confirmed
Anesthesia: Local infiltration with ***
Approach: Wound prepped, cleansed, and copiously irrigated with normal saline under high pressure.
Exploration: Wound explored to galea — no skull fracture, no foreign body.
Methods: Closed with *** staples. Hemostasis achieved.
Complications: None. Patient tolerated procedure well.
Clinical Education
Suture Selection by Location
| Location | Skin | Deep | Notes |
| Face | 6-0 nylon or fast-absorbing gut | 5-0 Vicryl | Cosmesis priority. Remove 4-5 days |
| Scalp | Staples (or 3-0 nylon) | 3-0 Vicryl (if galea repair) | Hair apposition technique for small wounds |
| Extremity | 4-0 nylon (arm/leg), 5-0 (hand/foot) | 4-0 Vicryl | Remove 7-10 days; 12-14 over joints |
| Trunk | 3-0 or 4-0 nylon | 3-0 or 4-0 Vicryl | Remove 7-10 days |
| Tongue / oral | 4-0 or 5-0 Vicryl or chromic gut | — | Absorbable only. Loose bites |
Suture Material Properties
| Material | Type | Tensile Strength | Absorption | Use |
| Nylon (Ethilon) | Non-absorbable | Excellent, retains long-term | N/A — requires removal | Workhorse for skin closure |
| Prolene | Non-absorbable | Excellent, minimal memory | N/A — requires removal | Good for running/subcuticular; slick, easy removal |
| Vicryl | Absorbable, braided | 50% at 21 days | Complete by 56-70 days | Deep/dermal layer closure |
| Vicryl Rapide | Absorbable, braided | 50% at 5 days | Complete by ~14 days | Facial skin — no removal needed (peds-friendly) |
| Chromic Gut | Absorbable, monofilament | 50% at 10-14 days | Complete by ~90 days | Oral mucosa, peds face, areas where removal is difficult |
| Fast-Absorbing Gut | Absorbable, monofilament | 50% at 5-7 days | Complete by 14-28 days | Face (skin), peds — falls off on own |
Suture Removal Timeline
| Location | Days |
| Eyelid | 3-4 |
| Face, neck | 4-5 |
| Scalp, trunk, extremity | 7-10 |
| Palms, soles, over joints | 12-14 |
Anesthesia Pearls
LET gel (lidocaine-epi-tetracaine): Apply to open wound x 20-30 min. Excellent for face and scalp lacerations in peds. Do NOT use on digits, nose tip, ears, or penis (end-artery concern, though epinephrine in digital blocks is now considered safe).[3]
Buffered lidocaine: 9:1 ratio of lidocaine to sodium bicarbonate (8.4%). Dramatically reduces injection pain. Should be standard practice for all local infiltration.[4]
Digital block: 1-2mL lidocaine (without epi is traditional; with epi is now considered safe) at the 2 and 10 o’clock positions of the digital web space. Faster onset than traditional two-injection technique.[3]
Intranasal options (peds): Fentanyl 1-2 mcg/kg IN (max 1mL per nostril) or midazolam 0.3-0.5mg/kg IN for anxiolysis before local. Onset 5-10 min.
Wound Closure Timing
The “golden period” of 6 hours is a myth. Evidence supports primary closure of clean wounds up to 18-24 hours after injury for most locations. Face and scalp can often be closed even later given rich blood supply and low infection rates.[5]
Leave open: Heavily contaminated wounds (bites, crush, soil), puncture wounds, wounds with significant devitalized tissue, and delayed presentations with signs of infection. Pack, allow healing by secondary intention, delayed primary closure at 3-5 days if clean.
Antibiotics in Lacerations
Most lacerations do NOT need antibiotics. Consider prophylactic antibiotics for: bite wounds (dog, cat, human — especially hand bites), crush injuries, heavily contaminated wounds, open fractures, immunocompromised patients, and wounds with significant devitalized tissue.[6]
Bite wounds: Augmentin 875mg BID x 5-7 days (Clindamycin + fluoroquinolone if PCN allergy). Cat bites have highest infection rate (~50%) due to deep puncture inoculation — treat prophylactically. Dog bites: prophylactic antibiotics for hand/foot bites, crush injuries, or immunocompromised; other locations can be managed with close follow-up alone.[6]
Tetanus: Give Tdap if >5 years since last booster for dirty/contaminated wounds, >10 years for clean wounds, or unknown vaccination history. Add TIG (tetanus immune globulin) if ❤ lifetime doses and dirty wound.
High-Risk Wounds
Tendon injury: Test function against resistance in full ROM — partial lacerations can have intact function at rest. Extensor tendons can often be repaired in ED; flexor tendon injuries require hand surgery referral. Any tendon injury over MCP joint from a fist-to-tooth (“fight bite”) — assume joint capsule violation until proven otherwise.[7]
Nerve injury: Test two-point discrimination (normal <5mm in fingertip) and light touch in autonomous zones. Document before anesthesia. Complete lacerations of digital nerves in fingers warrant microsurgical referral.
Joint capsule violation: If wound overlies a joint — explore to depth. Saline load test (inject sterile saline into joint, watch for extravasation from wound) if concern. If positive — washout and orthopedics/hand surgery consult.[7]
Tongue Laceration Pearls
Most tongue lacs heal without repair — oral mucosa has excellent blood supply and rapid epithelialization. Repair if: gaping, on the tongue margin/tip, through-and-through, bisecting, or actively bleeding after pressure.[2]
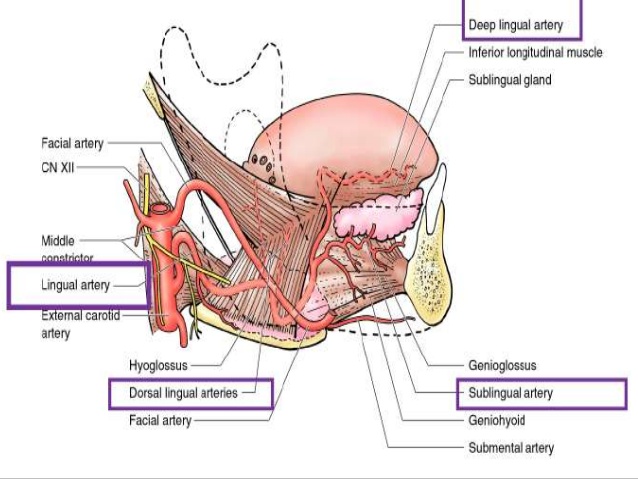
Lingual artery: Deep midline tongue lacerations can injure the lingual artery (see anatomy above). If significant hemorrhage — direct pressure, figure-of-eight deep suture. If uncontrollable, ENT consult and possible angiographic embolization.
References
- Singer AJ et al. Evaluation and Management of Traumatic Lacerations. NEJM. 1997;337(16):1142-1148. PubMed
- Zehtabchi S et al. Management of Lacerations Involving the Tongue. Ann Emerg Med. 2015;65(4):389-395. PubMed
- Ilicki J. Safety of Epinephrine in Digital Nerve Blocks: A Literature Review. J Emerg Med. 2015;49(5):799-809. PubMed
- Cepeda MS et al. Alkalinization of Local Anesthetics to Reduce Pain on Infiltration. Cochrane Database Syst Rev. 2010;(12):CD006581. PubMed
- Quinn JV et al. Traumatic Lacerations: What Are the Risks for Infection and Has the “Golden Period” of Laceration Care Disappeared? Emerg Med J. 2014;31(2):96-100. PubMed
- Stevens DL et al. IDSA Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update. Clin Infect Dis. 2014;59(2):e10-e52. PubMed
- Patel L, Gross J. Management of Complex Hand Lacerations in the Emergency Department. Emerg Med Pract. 2020;22(10):1-24. PubMed
