ICD/Pacemaker Problems
ICD/Pacemaker Problems MDM
Last reviewed: March 2026
Contents
MDM Templates
ICD/Pacemaker — Early Complication
Patient presents with *** following recent device implantation (*** days post-implant). Early complications including infection, lead displacement, pneumothorax, and hematoma are on the differential. Patient’s presentation with *** and exam findings of *** are concerning for ***. Workup demonstrates ***.
History, exam, and imaging reassure against other etiologies. Device interrogation obtained if immediate life threat not present — specific findings documented per cardiology review.
If infection suspected (fever, erythema, purulence, erosion): Blood cultures obtained. Cardiology and infectious disease consulted regarding need for device removal and staged reimplantation. Broad-spectrum antibiotics initiated after cultures, pending identification.
If lead displacement: ECG obtained to confirm loss of pacing capture. Cardiology notified emergently — may require fluoroscopic repositioning. Patient admitted for monitoring and intervention.
If pneumothorax: Chest imaging obtained. Size assessed. If small (<2 cm) and asymptomatic, observation with repeat imaging at 6 hours may be appropriate pending cardiology input. Larger pneumothorax or hemodynamic compromise requires intervention.
If hematoma: Assess for active bleeding, signs of infection, or compartment syndrome. Large expanding hematomas may require evacuation. Anticoagulation held if patient on anticoagulation for device indication.
Plan: Cardiology and appropriate specialists consulted. Disposition: Admit for monitoring, further imaging, device interrogation, and intervention as indicated.
ICD/Pacemaker — Late Complication
Patient with remote device history (*** years post-implant) presents with *** suggestive of late device complication. Differential includes lead fracture, generator malfunction, pocket infection, and lead perforation. Physical exam reveals ***. ECG shows ***.
History and workup establish the likely etiology. Pocket imaging obtained if infection suspected. Lead integrity assessed by device interrogation if malfunction is concern.
If pocket infection (erythema, drainage, erosion): Blood cultures obtained. Device removal indicated — either emergent if hemodynamically unstable or urgent staged removal with lead extraction. Antibiotic course typically extends 4-6 weeks post-removal before reimplantation. Broad-spectrum coverage initiated after cultures pending culture results and species identification.
If lead fracture (loss of capture, failure to sense, inability to pace): Cardiology consulted for lead revision. May be urgent or semi-urgent depending on patient’s underlying rhythm and pacing dependence. Temporary pacing may be needed if patient pacing-dependent and waiting for intervention.
If generator malfunction: Cardiology consulted. Battery depletion is managed by elective generator replacement. True hardware malfunction may require emergent intervention or temporary pacing depending on severity and patient’s intrinsic rhythm.
If lead perforation (acute onset pericardial effusion with hemodynamic compromise): Emergent cardiothoracic and cardiology consultation. May require urgent intervention or surgery. Hemodynamic monitoring and preparation for pericardiocentesis if tamponade develops.
Plan: Cardiology consulted emergently if hemodynamically unstable or signs of life threat. Device interrogation obtained. Disposition: Admit for intervention, monitoring, and specialist care.
ICD Shocks — Appropriate and Inappropriate
Patient with ICD history presents following one or more shocks. Determine whether shocks are appropriate (in response to device-detected ventricular arrhythmia) or inappropriate (triggered by sinus tachycardia, SVT, T-wave oversensing, or lead malfunction). Obtain device interrogation with rhythm strip during shock. Correlate with clinical presentation and ECG findings.
If appropriate shock(s): Device functioned as programmed. Review recent symptoms, precipitants, and medication/electrolyte status. Assess for arrhythmia trigger — ACS, electrolyte derangement, myocarditis, worsening heart failure. Workup accordingly. Consider amiodarone or beta-blocker optimization if recurrent appropriate shocks. Cardiology consultation for device programming review and medication adjustment. Disposition determined by underlying etiology and frequency of events.
If inappropriate shock(s): Determine mechanism — SVT, sinus tachycardia with double-counting, T-wave oversensing, lead malfunction. Chest X-ray obtained to assess for lead fracture. Device interrogation reviewed for signal noise, impedance abnormalities. Cardiology consulted for programming adjustment or device revision if lead integrity compromised. Disposition: Admit if multiple inappropriate shocks (risk of recurrence), or discharge with urgent cardiology follow-up if isolated event with clear reversible cause and corrected programming.
If ≥3 appropriate shocks in 24 hours (electrical storm): This is a medical emergency. Obtain ECG and device interrogation. Initiate aggressive beta-blocker (metoprolol IV or oral, or esmolol IV infusion if hemodynamically unstable), add amiodarone IV loading. Sedate if conscious. Consider application of magnet to temporarily disable tachyarrhythmia therapy while medical management takes effect — magnet does NOT stop pacing, only prevents shock delivery. Intensive care admission. Identify and treat underlying arrhythmia trigger. Cardiology consulted emergently for device reprogramming, possible catheter ablation, and management optimization.
Plan: Device interrogation reviewed. Cardiology consulted. Disposition: Admit (ICU if electrical storm). Discharge with urgent cardiology follow-up only if isolated event with documented benign etiology and normal device function.
Pacemaker Malfunction
Patient with pacemaker presents with *** concerning for device malfunction. Obtain 12-lead ECG to assess for pacing spikes, capture, and sensing. Correlate with patient’s underlying rhythm and programmed rate. Device interrogation obtained to confirm malfunction and identify specific problem.
If failure to pace (no pacing spike when expected): Causes include oversensing (sensing electrical noise or myopotentials, suppressing pacing), lead displacement, lead fracture, battery depletion, loss of capture threshold, or connector malfunction. Check ECG for native rhythm — patient may be protected if intrinsic rate adequate. If patient is pacing-dependent and has failed to pace, this is a medical emergency. Magnet application may restore asynchronous pacing while preparing for intervention. Cardiology consulted emergently. Temporary pacing may be needed. Disposition: Admit with urgent device intervention.
If failure to capture (pacing spikes present but no QRS follows): Causes include lead displacement, elevated capture threshold, lead fracture, metabolic derangement (severe hyperkalemia), or increasing pacing impedance. Check electrolytes — hyperkalemia must be corrected emergently. Assess for mechanical cause by imaging. If patient is pacing-dependent and there is no intrinsic escape rhythm, this is a life threat. Temporary pacing arranged urgently. Cardiology consulted for lead revision or adjustment of pacing parameters. Disposition: Admit.
If failure to sense (device does not see native beats, causing competitive pacing): Undersensing causes include lead displacement, lead fracture, signal amplitude decline, or programming sensitivity set too high (insensitive). Risk of R-on-T pacing precipitating dangerous arrhythmia. ECG may show pacing spikes falling on native QRS or T-wave, creating fusion or pseudofusion beats and risk of PVC/VF induction. Check electrolytes — severe hyperkalemia may blunt QRS amplitude. Cardiology consulted for device reprogramming (increase sensitivity) or lead revision if structural problem. Disposition: Admit if failure to sense confirmed or if patient has had symptoms (palpitations, syncope). Semi-urgent follow-up if isolated finding without symptoms.
Plan: ECG obtained. Electrolytes checked including potassium. Device interrogation reviewed by cardiology. Cardiology consulted emergently if failure to pace or capture with pacing dependence. Specific intervention (lead revision, generator replacement, parameter adjustment) determined by interrogation findings and cardiology assessment. Disposition: Admit if malfunction with hemodynamic consequence or pacing dependence, or if patient pacing-dependent with failed backup rhythm.
Clinical Education
Device Basics and NBG Code
Pacemakers versus ICDs: Pacemakers provide electrical stimulation to restore or maintain adequate heart rate. ICDs incorporate pacemaker function plus the ability to detect and terminate dangerous arrhythmias through overdrive pacing or shock delivery. Both devices consist of a pulse generator (battery and circuitry) housed in the chest pocket, connected to one or more leads that rest in or on the heart.
Device types: Single-chamber devices (VVI or AAI) pace or sense in one chamber only. Dual-chamber devices (DDD or similar) pace/sense in both atrium and ventricle, allowing AV synchrony. Biventricular or CRT (cardiac resynchronization therapy) devices pace both ventricles plus the right atrium, designed for patients with significant left ventricular dysfunction and conduction delay.
NBG Code: Device programming is summarized by the three-letter NBG (NASPE/BPEG) code. Position 1 = chamber paced (V, A, or D for both). Position 2 = chamber sensed (V, A, or D). Position 3 = response to sensed event (I = inhibited [sensing suppresses pacing], T = triggered [sensing causes pacing], D = dual [both I and T functions]). Example: DDD pacemaker paces and senses in both chambers and responds to sensing in both chambers. VVI pacemaker paces and senses in ventricle only, and sensed beats inhibit (suppress) pacing.
You do not need to understand every nuance of programming — the key is recognizing when a pacing spike appears or disappears when it should or shouldn’t, and understanding the three main failure modes: failure to pace, failure to capture, and failure to sense.
Failure to Pace
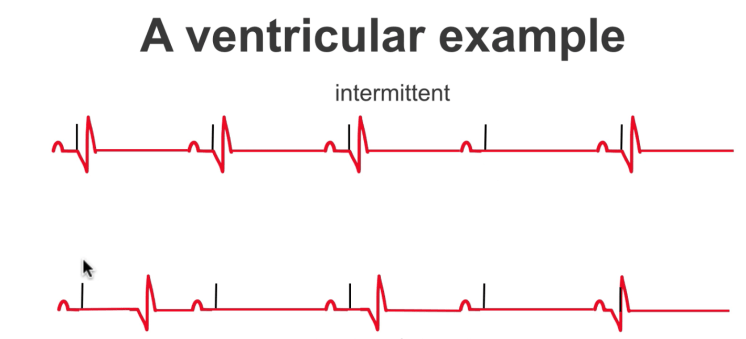
Failure to pace means no pacing spike appears when the device should be pacing. On ECG, you expect to see a short vertical line (pacing spike) before each QRS in the paced chamber. If spikes disappear when they should be present, the device has failed to sense the native rhythm (oversensing) or has another problem preventing output.
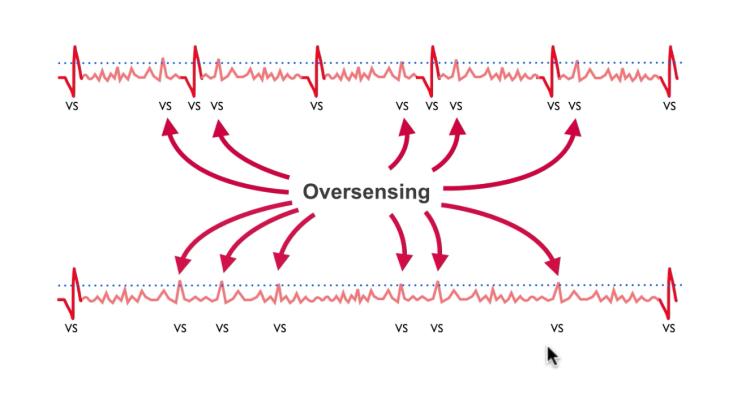
Oversensing is the most common cause. The device incorrectly senses electrical noise and interprets it as a native heartbeat, suppressing pacemaker output. Common causes include electromagnetic interference (EMI) from equipment in the ED or home, myopotentials from skeletal muscle contraction (vigorous coughing, shoulder shrugging), or inappropriate sensing of the T-wave (T-wave oversensing). Lead fracture can cause intermittent contact and signal noise, triggering oversensing.
If a patient is pacing-dependent and oversensing causes failure to pace, the patient loses all pacemaker support. This is a medical emergency. Applying a magnet directly over the device generator converts most pacemakers to asynchronous pacing at a fixed rate (typically 80-100 bpm), temporarily bypassing the sensing circuit. This “asynchronous” mode ignores native rhythm and paces at the set rate regardless, ensuring output while you arrange definitive intervention. Device interrogation and lead imaging follow to identify and correct the problem.
Failure to Capture
Failure to capture means pacing spikes appear but the heart does not depolarize in response. On ECG, you see the pacing artifact but no QRS follows — the spike does not “capture” the myocardium into contraction.
Lead displacement is the most common cause, especially in the early post-implant period. If the lead tip shifts away from the endocardium, electrical contact is lost and the stimulus cannot depolarize the chamber. Other causes include elevated capture threshold (the amount of electrical energy needed to depolarize myocardium; thresholds rise over time as scar forms around the lead), lead fracture, severe metabolic derangement (especially hyperkalemia, which raises the threshold), and increasing pacing impedance from device malfunction.
Hyperkalemia specifically: Severe hyperkalemia blunts the QRS and raises capture thresholds, making it harder for the device to depolarize tissue. Correct hyperkalemia emergently — this may restore capture even if the lead position is unchanged.
If failure to capture occurs and the patient has no intrinsic escape rhythm (i.e., patient is pacing-dependent), the patient loses cardiac output. This is a cardiac emergency. Temporary pacing must be arranged immediately. Cardiology consulted emergently for lead revision or device parameter adjustment. Disposition is hospital admission.
Failure to Sense
Failure to sense means the device does not detect native heartbeats, so the sensing circuit does not suppress (inhibit) pacemaker output. The device continues to pace despite the presence of adequate native rhythm, leading to competitive pacing where device output and native beats occur independently.
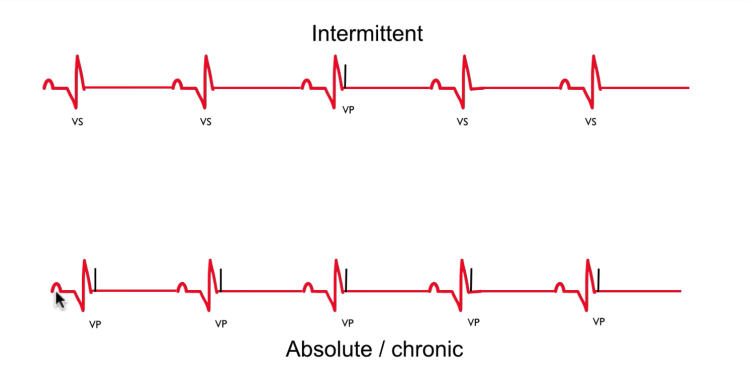
The danger of failure to sense is R-on-T pacing: If a pacing spike falls on the native T-wave, it can trigger ventricular fibrillation. Even if no arrhythmia occurs, competitive pacing creates fusion beats (partly paced, partly native) and pseudofusion beats (paced beat on top of native activity). These look abnormal and can be mistaken for ectopy.
Causes of undersensing include lead displacement, lead fracture, loss of signal amplitude (as the lead ages), or programming sensitivity set too high (insensitive — the device looks for large signals and misses smaller native beats). Severe hyperkalemia may also blunt QRS amplitude enough that the device undersenses.
Management includes correcting severe electrolyte abnormalities (especially hyperkalemia), checking lead integrity by imaging and device interrogation, and reprogramming sensitivity (increase sensitivity = look for smaller signals = better sensing). If a structural lead problem is found, lead revision may be needed.
Magnet Behavior
Magnet application over a pacemaker converts it to asynchronous (fixed-rate) pacing. The magnet disables the sensing circuit, so the device ignores all native rhythm and paces at a preset rate (usually 80-100 bpm) regardless of what the heart is doing. This ensures output if sensing has failed.
Magnet application over an ICD is different: It disables tachyarrhythmia therapies (prevents shocks) but does NOT turn off pacing. The ICD continues to pace normally if the patient is pacing-dependent. The magnet essentially says to the ICD, “You can still pace, but no shocks.” This is critical during electrical storm or after multiple inappropriate shocks — applying the magnet gives you time to treat the underlying arrhythmia while preventing further shocks.
Critical point: Magnet does NOT turn off pacing on either device. It affects sensing (pacemakers) or shock delivery (ICDs), but output pacing continues or is restored.
Magnet effects are temporary — once the magnet is removed, normal function resumes. Always arrange definitive device interrogation and intervention while the magnet is in place.
Electrical Storm
Electrical storm is ≥3 appropriate ICD shocks within 24 hours. It represents a dangerous state of recurrent ventricular arrhythmia despite ICD therapy and requires immediate aggressive intervention.
Mechanism: An underlying arrhythmia trigger (ACS, myocarditis, electrolyte abnormality, device malfunction, or worsening heart failure) causes repeated ventricular arrhythmia. Each time the device detects VT/VF, it delivers a shock. But the underlying cause is not addressed, so another arrhythmia occurs, and the cycle repeats. The patient is shocked repeatedly, conscious episodes are terrifying, sedatives may not prevent awareness of shocks, and the repeated trauma depletes the ICD battery.
ED management: This is a medical emergency requiring ICU admission. Obtain a 12-lead ECG and device interrogation to confirm appropriate shocks and rule out device malfunction. Start aggressive medical therapy: load amiodarone IV (300 mg over 20-60 minutes, then continuous infusion), maximize beta-blocker (IV metoprolol or esmolol if hemodynamically precarious). If the patient is conscious and distressed, sedate with benzodiazepine (midazolam or lorazepam IV). Identify the underlying trigger — check troponin, electrolytes (especially potassium), ECG for ischemic changes, assess for myocarditis symptoms or heart failure decompensation.
Magnet use: While medical management is being arranged, applying a magnet over the ICD disables shock delivery. The device continues to pace but will not shock, giving you time to optimize medical therapy before shocks resume. This is a temporary measure — the underlying arrhythmia trigger must be identified and treated. Once the patient is stable on medications and trigger is addressed, remove the magnet and reprogram the device as needed.
After stabilization, consider catheter ablation (electrophysiology consult) if the arrhythmia substrate is accessible. Cardiology and intensive care team involved throughout.
Pacemaker-Mediated Tachycardia
Pacemaker-mediated tachycardia (PMT) is a reentrant loop that occurs in dual-chamber pacemakers. The mechanism is: (1) A premature ventricular beat occurs. (2) The PVC conducts retrograde up the AV node to the atrium (invisible on ECG), depolarizing the atrial lead. (3) The atrial lead senses this retrograde P-wave. (4) According to the device programming (typically DDD mode), sensing a P-wave triggers a ventricular pace after the AV delay. (5) The paced ventricular beat again conducts retrograde to the atrium, creating another P-wave sensation, and the cycle continues. The result is a regular tachycardia (usually 120-160 bpm) with a 1:1 AV relationship on ECG.
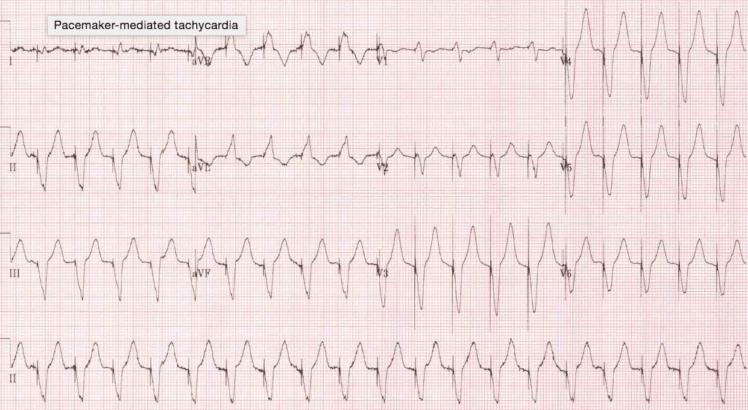
Clinical presentation: Patient reports palpitations, regular at a rapid rate. PMT is not dangerous in the sense that it does not cause cardiogenic shock (it is a regular rhythm with intact AV synchrony), but it is uncomfortable and depletes the battery faster.
Management: Applying a magnet over the pacemaker breaks the reentrant circuit by converting to asynchronous pacing, which stops the tachycardia immediately. Once the magnet is removed, normal function resumes, but PMT may recur. Cardiology consulted to reprogram the device — strategies include shortening the post-ventricular atrial refractory period (PVARP) so the retrograde P-wave falls in the refractory period and is not sensed, or enabling PMT prevention algorithms that are built into most modern devices.
Modified Sgarbossa Criteria with Paced Rhythm
Interpreting STEMI in a patient with a paced rhythm is challenging because the paced QRS is wide and already shows discordant ST-T changes. The modified Sgarbossa criteria help identify true STEMI in the presence of pacing.
The three criteria are exactly the same as the LBBB criteria (since both have wide QRS and ventricular depolarization first): (1) Concordant ST elevation ≥1 mm in leads with positive QRS. (2) Concordant ST depression ≥1 mm in leads V1-V3. (3) Discordant ST elevation ≥25% of the QRS amplitude in leads with negative QRS.
Application: If any one of these three is present in a paced patient with chest pain, STEMI is likely and the patient needs emergent cardiology consultation and consideration for acute reperfusion. The criteria are not perfectly sensitive or specific, but they help avoid missing acute MI in this difficult population.
In the paced patient with chest pain and no Sgarbossa criteria met, the diagnosis of acute MI is not ruled out — serial ECGs and troponin are still essential. But presence of one or more Sgarbossa criteria significantly raises MI probability.
References
- Strickberger SA, Daoud EG, Cheung R. Implantable cardioverter-defibrillators. Lancet. 2005;365(9465):1141-1149. PubMed
- Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management. Heart Rhythm. 2009;6(7):1085-1104. PubMed
- Zipes DP, Link MS, Ackerman MJ, et al. 2015 ACC/AHA/HRS focused update of the 2010 guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol. 2016;68(25):e91-e141. PubMed
- Sideris A, Archontakis S, Dilaveris PE, Gialafos EJ, Toutouzas PK. Pacemaker-mediated tachycardia: incidence, mechanism, and prevention. Pacing Clin Electrophysiol. 2006;29(4):408-424. PubMed
- Kusumoto FM, Schoenfeld MH, Wilkoff BL, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. J Am Coll Cardiol. 2019;74(1):104-132. PubMed
- Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. N Engl J Med. 1996;334(8):481-487. PubMed
- Josephson ME, Callans DJ. Using the electrocardiogram to diagnose disorders of arrhythmia mechanisms. Circulation. 2013;128(22):2457-2481. PubMed
- Swerdlow CD, Wang PJ, Zipes DP. Pacemakers and implantable cardioverter-defibrillators: mechanisms and management. J Am Coll Cardiol. 2016;67(25):3035-3050. PubMed
