Last reviewed: March 2026
Contents
MDM Templates
Bite Wound — Simple
Patient presents with a bite wound from a ***. Based on history, exam, and any testing performed, there does not appear to be a retained foreign body, nerve injury, vascular injury, tendon injury, or bone involvement. Wound irrigated copiously.
Given the wound characteristics and risk factors, prophylactic antibiotics initiated.
Plan: Amoxicillin-clavulanate 875/125 mg PO BID for 5 days. Wound care instructions. Tetanus updated.
Disposition: Discharge with return precautions for worsening redness, swelling, purulent drainage, red streaking, or fever. Follow up with PCP within 48 hours for wound check.
Bite Wound — Hand (Fight Bite)
Patient presents with a wound to the hand over the MCP joint consistent with a clenched-fist injury (fight bite). Neurovascular and tendon exam intact. No signs of joint capsule violation, tendon injury, or deep space infection on exam.
This wound has high risk for joint space violation and deep infection given the mechanism. Wound irrigated extensively. Imaging obtained to evaluate for fracture, foreign body, and joint space gas.
Plan: Amoxicillin-clavulanate 875/125 mg PO BID for 7 days. Wound left open — not closed primarily. Splint for comfort.
Disposition: Discharge with 24-hour wound check and hand surgery follow-up within 48 hours. Return immediately for worsening swelling, inability to move fingers, or fever.
If joint capsule violated or signs of infection:
Hand surgery consulted for operative irrigation and debridement. IV antibiotics initiated.
Bite Wound — Complex / Deep
Patient presents with a bite wound with deep tissue involvement. Wound reaches the level of muscle, tendon, or involves the joint capsule. Wound irrigated extensively.
Given depth of wound and involvement of deep structures, patient at high risk for deep infection.
Surgery consulted: Regarding wound depth, need for operative irrigation and debridement, and disposition.
Plan: IV antibiotics. Wound left open.
Disposition: Per surgical recommendation.
Clinical Education
Antibiotic Indications
Not all bite wounds need antibiotics — but most high-risk ones do. Antibiotics are indicated for: wounds to the hand (highest infection risk), wounds reaching muscle or tendon, joint capsule violation, cat bites (deep puncture inoculation), human bites, immunocompromised patients, crush injuries, and wounds presenting >12 hours after injury. Superficial dog bites to the extremities (not the hand) in immunocompetent patients can often be managed with wound care alone.[1]
First-line: amoxicillin-clavulanate 875/125 mg BID. This covers the polymicrobial flora of bite wounds — Pasteurella (cats/dogs), Eikenella (humans), streptococci, staphylococci, and anaerobes. For penicillin allergy: doxycycline or TMP-SMX + metronidazole, or moxifloxacin as monotherapy.
Microbiology by Bite Type
| Bite Type | Key Organisms | Notes |
| Dog | Pasteurella, strep, staph, Capnocytophaga | Capnocytophaga can cause overwhelming sepsis in asplenic/immunocompromised |
| Cat | Pasteurella multocida (75%), strep, staph | Deep puncture → high infection rate (30–50%) |
| Human | Eikenella corrodens, strep, staph, anaerobes | Polymicrobial; fight bites over MCP joint are joint emergencies |
Wound Management
Irrigate aggressively — this is the most important intervention. High-pressure irrigation with normal saline (18-gauge needle on a 30–60 mL syringe) significantly reduces infection rates. Puncture wounds (cat bites) are hard to irrigate effectively, which is one reason they have higher infection rates.[2]
Primary closure is acceptable for most dog bite lacerations to the face — cosmesis matters and infection rates are low with irrigation and antibiotics. Do NOT close: hand bites, crush injuries, puncture wounds, wounds >12 hours old (>24 hours for face), and human bites. These should be left open for healing by secondary intention or delayed primary closure.
Rabies Prophylaxis
The decision is about the animal, not the wound. Consider rabies prophylaxis for bites from bats (any contact — even waking up in a room with a bat), raccoons, skunks, foxes, and unvaccinated/stray dogs or cats. The virus travels ~7 cm/day toward the spinal cord and then rapidly to the brain — bites to the face and hands have the shortest incubation period.[3]
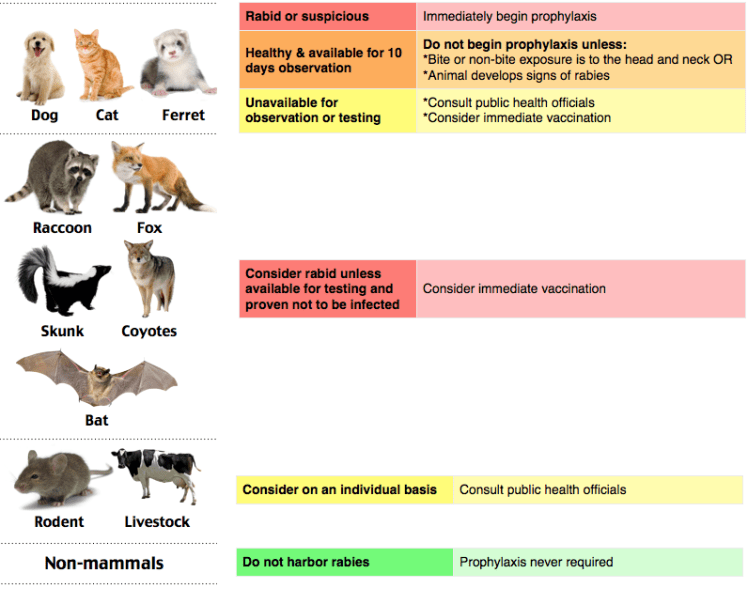
Rabies post-exposure prophylaxis algorithm
Post-exposure prophylaxis: RIG 20 IU/kg infiltrated around the wound site (the full dose should go around the wound if anatomically feasible). Rabies vaccine 1 mL IM on days 0, 3, 7, and 14 in the contralateral deltoid. For immunocompromised patients, add a 5th dose on day 28.
Cat Bite Pearls
Cat bites have infection rates of 30–50% — significantly higher than dog bites (~5–15%). Cat teeth are thin and sharp, creating deep puncture wounds that inoculate bacteria directly into tendons, joints, and bone. Pasteurella multocida is the dominant organism and causes rapid-onset infection (often within 12–24 hours of the bite). All cat bites should receive prophylactic antibiotics.[4]
Human Bite / Fight Bite Pearls
The fight bite (clenched-fist injury) is the most dangerous human bite. The tooth penetrates the extensor tendon and joint capsule over the MCP joint while the fist is clenched. When the hand opens, the skin wound migrates away from the underlying tendon and joint injury — hiding the depth of penetration. Always examine the hand in both the open and clenched position. If there’s any chance of joint violation, treat it as an open joint.[5]
Blood-borne pathogen counseling: HIV and hepatitis B/C transmission from human bites is theoretically possible but exceedingly rare. The risk from a bite is much lower than from a needlestick. Follow institutional guidelines for exposure evaluation, but reassure the patient that the risk is very low.
References
- Baddour LM et al. Management of bite wounds and infection. UpToDate. Reviewed 2024.
- Maimaris C, Quinton DN. Dog-bite lacerations: a controlled trial of primary wound closure. Arch Emerg Med. 1988;5(3):156-161. PubMed
- Manning SE et al. Human rabies prevention — United States, 2008: recommendations of the ACIP. MMWR Recomm Rep. 2008;57(RR-3):1-28. PubMed
- Talan DA et al. Bacteriologic analysis of infected dog and cat bites. N Engl J Med. 1999;340(2):85-92. PubMed
- Kennedy SA et al. Human and other mammalian bite injuries of the hand: evaluation and management. J Am Acad Orthop Surg. 2015;23(1):47-57. PubMed
