Last reviewed: March 2026
Contents
MDM Templates
Minor Burn — Discharge
Patient presents with a burn sustained from ***. Airway is intact with no evidence of inhalation injury — no singed nasal hairs, no carbonaceous sputum, no stridor, no facial burns. Burns are partial thickness involving less than 10% TBSA, not involving the face, hands, feet, genitalia, or major joints, and not circumferential.
History and exam lower suspicion for inhalation injury, full-thickness burns requiring grafting, circumferential burns with compartment risk, or concomitant trauma. Patient does not meet ABA burn center referral criteria.
Plan: Wound cleansed, debrided of loose tissue, dressed with Mepilex or xeroform with bacitracin. Tetanus updated. Pain controlled with oral analgesics.
Disposition: Discharge with wound care instructions, return precautions for increasing pain, spreading redness, fever, or purulent drainage. PCP or wound care follow-up within 48 hours.
Major Burn — Burn Center Transfer
Patient presents with a burn sustained from *** with findings meeting ABA burn center referral criteria. Airway assessed and is currently intact / required intubation for airway protection given concern for inhalation injury.
Burn characteristics and extent meet criteria for burn center transfer. History and exam raise concern for significant partial or full-thickness burns requiring specialized wound management, possible grafting, and multidisciplinary burn care.
Plan: IV fluid resuscitation initiated per Parkland formula guidance. Wound dressed. Pain managed with IV opioid analgesia. Tetanus updated. Burn center contacted and accepting transfer.
Disposition: Transfer to burn center.
Admit if: Burns meeting burn center criteria but transfer not immediately available. ICU for inhalation injury, >20% TBSA, or hemodynamic instability.
Clinical Education
Burn Center Transfer Criteria
ABA referral criteria (any of the following): Partial thickness burns >10% TBSA, full-thickness burns of any size, burns to face/hands/feet/genitalia/perineum/major joints, chemical burns, electrical burns (including lightning), inhalation injury, burns with concomitant trauma where the burn is the greater risk, burns in patients with significant comorbidities, burns in children at hospitals without qualified pediatric burn care.[1]
Fluid Resuscitation
Parkland formula: 4 mL x kg x %TBSA burned. Give half in the first 8 hours from time of burn (not time of arrival), remaining half over the next 16 hours. Initiate for burns >20% TBSA.[2] MDCalc: Parkland Formula
Practical pearls: The Parkland formula is a starting point, not a target. Many burn centers now cap initial rates at 500 mL/hr to avoid over-resuscitation (“fluid creep”), which causes abdominal compartment syndrome, extremity compartment syndrome, and pulmonary edema. Titrate to urine output 0.5-1 mL/kg/hr in adults.[2]
Wound Care & Dressings
| Dressing | Use | Pearl |
| Mepilex Ag / Mepilex Transfer | Partial thickness burns | Can be left intact 3-7 days. Less painful dressing changes. Preferred by most burn centers. |
| Xeroform + bacitracin | Partial thickness burns | Traditional option. Change daily. Cover with dry gauze. |
| Silver sulfadiazine (Silvadene) | Deep partial / full thickness | Avoid in superficial partial thickness burns — inhibits keratinocyte migration and delays healing. Also avoid on face. |
Key wound care steps: Cool running water for 20 minutes (within 3 hours of burn). Debride loose blisters (intact tense blisters can be left). Do not apply ice. Do not apply butter or toothpaste (yes, patients still do this).[3]
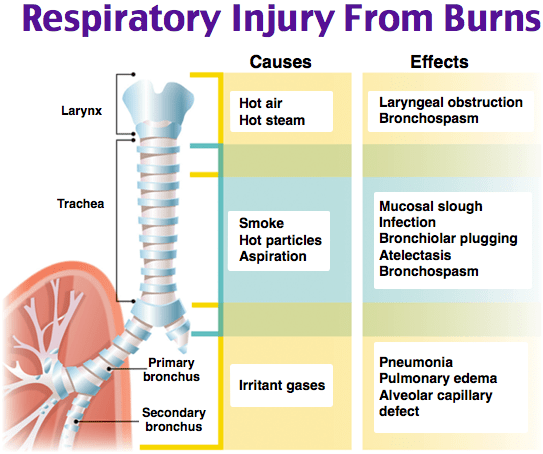
Inhalation Injury
Suspect inhalation injury with: enclosed-space fire, facial burns, singed nasal hairs/eyebrows, carbonaceous sputum, hoarseness, stridor, or hypoxia. Inhalation injury is the strongest independent predictor of burn mortality.[4]
Intubate early if you suspect it. Airway edema progresses rapidly with fluid resuscitation. If you’re thinking about intubation at hour 1, the patient will need it at hour 3. Don’t wait for desaturation.
CO poisoning: Check carboxyhemoglobin on all fire victims. SpO2 is unreliable — it reads falsely normal. Treat with 100% FiO2 via NRB. Consider hyperbaric oxygen for COHb >25%, loss of consciousness, or pregnancy.
Burn Centers (Los Angeles Area)
| Center | Contact |
| Grossman Burn Center (Santa Ana) | (714) 956-2876 or (818) 981-2050 |
| LAC+USC Regional Burn Center | (323) 226-7991 |
References
- American Burn Association. Burn Center Referral Criteria. ABA
- Baxter CR. Fluid Volume and Electrolyte Changes of the Early Postburn Period. Clin Plast Surg. 1974;1(4):693-703. PubMed
- Lexchin JR et al. Emergency Department Management of Minor Burns. Emerg Med Clin North Am. 2007;25(1):135-146. PubMed
- Walker PF et al. Diagnosis and Management of Inhalation Injury: An Updated Review. Crit Care. 2015;19:351. PubMed
