Tachydysrhythmias
Last reviewed: March 2026
Quick Links:
MDM Templates
Undifferentiated Tachycardia
Patient presents with palpitations and heart rate of *** bpm. Clinical exam reassuring with no evidence of hemodynamic compromise — blood pressure stable, no signs of acute heart failure, mental status intact. Deny chest pain, dyspnea, or syncope. History and preliminary workup do not suggest acute coronary syndrome, heart failure, or pulmonary embolism.
Rhythm classification on ECG consistent with *** [narrow regular / narrow irregular / wide complex]. Preliminary assessment lowers suspicion for life-threatening dysrhythmia. Troponin, basic metabolic panel, and thyroid function ordered to exclude precipitants including ACS, electrolyte derangement, and thyroid disease. ECG findings reviewed; no acute ischemic changes.
Plan: Continued cardiac monitoring while awaiting labs. Counseled on red-flag symptoms warranting immediate return (chest pain, dyspnea, syncope, severe palpitations). Depending on rhythm and response to observation, patient may benefit from beta-blocker or calcium channel blocker if sustained and symptomatic.
Disposition: Discharge home if vital signs remain stable, labs reassuring, and no concerning features on extended monitoring. Follow up with primary care for rate control optimization and outpatient stress testing if indicated by risk stratification. Return precautions emphasized.
Wide Complex Tachycardia / Ventricular Tachycardia
Patient presents with wide complex tachycardia on ECG at rate *** bpm. Hemodynamically stable with systolic blood pressure *** mmHg, no acute respiratory compromise, and clear mental status. Deny chest pain or severe dyspnea. History notable for ***. Assessment is consistent with ventricular tachycardia versus supraventricular tachycardia with aberrancy.
History, exam, and ECG features lower suspicion for acute coronary syndrome and severe heart failure. No signs of hyperkalemia, drug toxicity, or other metabolic derangement on initial assessment — electrolytes, troponin, and toxicology ordered. ECG reviewed for Brugada criteria (concordance, R-S interval, AV dissociation, morphology) to stratify VT versus SVT; pattern consistent with ***.
If ventricular tachycardia or high suspicion for VT: Plan: Amiodarone 150 mg IV load over 10 minutes, then continuous infusion at 1 mg/min for 6 hours, then reduce to 0.5 mg/min. Reassess at 1 hour; if rhythm persists, escalate to procainamide 10 mg/kg IV over 20 minutes. Continue monitoring and maintain IV access. If hemodynamics deteriorate or rhythm accelerates, proceed to synchronized cardioversion.
If SVT with aberrancy: Plan: Adenosine 6 mg IV rapid push, reassess; may repeat with 12 mg if no response. If adenosine ineffective or contraindicated, proceed to beta-blocker (metoprolol 2.5-5 mg IV) or calcium channel blocker (verapamil 2.5-5 mg IV titrated).
Disposition: Admit to ICU for continuous monitoring and antiarrhythmic titration. Cardiology consulted for ongoing management and consideration of electrophysiology study if recurrent or refractory. Electrolytes repleted as needed.
Ventricular Tachycardia Storm
Patient presents with recurrent or incessant ventricular tachycardia despite initial antiarrhythmic therapy. Multiple episodes over *** timeframe or failure to suppress with first-line agent (amiodarone). Hemodynamically unstable or episodes triggered by minimal activity / occur at rest. High-risk substrate evident — cardiomyopathy, prior MI, implantable device present, or acute ischemia.
Presentation consistent with VT storm — a life-threatening arrhythmia emergency defined by ≥3 episodes of sustained VT within 24 hours. Workup excludes reversible causes including acute MI, electrolyte derangement (magnesium, potassium, calcium), hypoxia, and drug toxicity. Underlying structural disease or prior arrhythmia history evident.
Plan: Aggressive escalation of antiarrhythmic therapy. Loading regimen: Amiodarone 150 mg IV over 10 minutes, then infusion at 1 mg/min × 6 hours. If persistent VT, escalate to procainamide 10 mg/kg IV over 20 minutes. If still refractory, add magnesium 2 g IV over 5-10 minutes. If hemodynamic instability or any concern for imminent collapse, proceed directly to synchronized cardioversion. Consider mechanical circulatory support (ECMO or intra-aortic balloon pump) if recurrent despite maximal medical therapy.
Adjunctive measures: Esmolol 500 mcg/kg/min IV infusion titrated for heart rate control and dysrhythmia suppression. Consider overdrive pacing (temporary pacing catheter) if available — rapid pacing may terminate refractory VT. Isoproterenol or high-dose epinephrine infusions have been used in specific scenarios (e.g., long-QT syndrome, bradycardia-dependent VT) under ICU/cardiology supervision. Stellate ganglion block considered if available for catecholaminergic VT or storm refractory to standard therapies.
Disposition: Immediate ICU admission with continuous telemetry, hemodynamic monitoring, and invasive arterial line. Early cardiology and electrophysiology consultation. Consider transfer to facility with extracorporeal membrane oxygenation (ECMO) capability if available locally or if refractory despite maximal therapy. Underlying cause identification and treatment urgent — acute MI requires revascularization, electrolyte repletion must be aggressive, arrhythmia device programming or implantation may be necessary.
Clinical Education
Tachycardia Classification: ECG-Based Approach
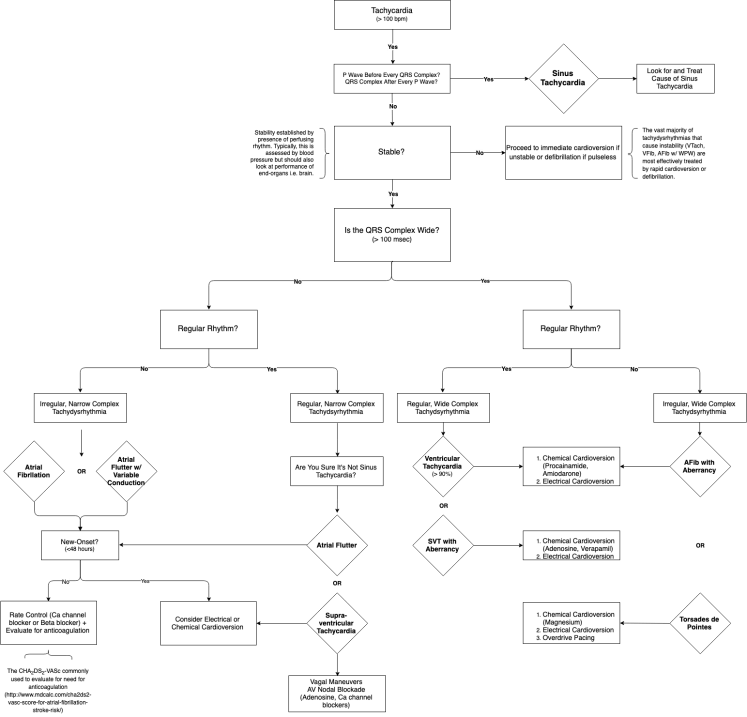
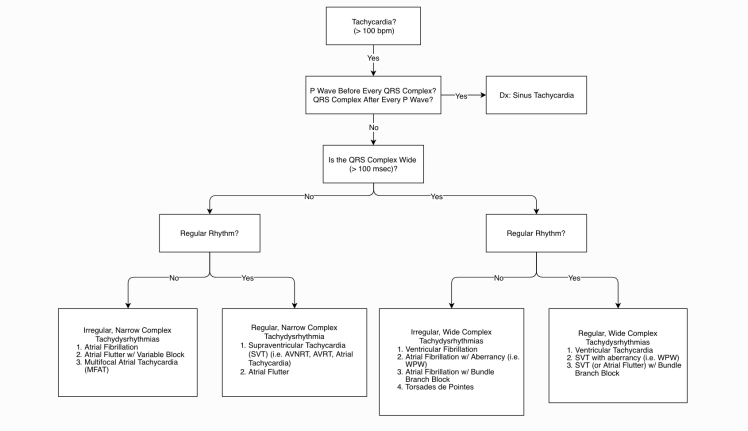
The first clinical decision point is to classify the tachycardia by QRS width and regularity on ECG. This immediately narrows the differential and guides initial therapy.
| Classification | QRS Width | Regularity | Common Etiologies |
| Narrow regular | <120 ms | Regular intervals | AVNRT, AVRT, sinus tachycardia, atrial flutter |
| Narrow irregular | <120 ms | Irregular intervals | Atrial fibrillation, multifocal atrial tachycardia, frequent PACs |
| Wide regular | >120 ms | Regular intervals | Ventricular tachycardia, SVT with aberrancy, SVT with accessory pathway |
| Wide irregular | >120 ms | Irregular intervals | AFib with rapid ventricular response, AFib with aberrancy, polymorphic VT/torsades |
High-yield pearl: Assume all wide complex tachycardias are VT until proven otherwise. VT is more common than SVT-with-aberrancy in the ED, and treating VT as SVT delays appropriate therapy and risks hemodynamic collapse. If in doubt, use antiarrhythmics safe for both (amiodarone, procainamide) rather than adenosine monotherapy [1].
Atrial Flutter: Recognition and Key Pearls
Atrial flutter is a regular narrow-complex tachycardia with characteristic “sawtooth” flutter waves in the baseline. The atrial rate is typically 250-350 bpm (most commonly ~300 bpm), but the ventricular rate depends on AV conduction. With 2:1 AV block, the ventricular rate is approximately 150 bpm; with 3:1 block, ~100 bpm; with 1:1 conduction (rare, dangerous), rates may exceed 300 bpm.
Identifying flutter waves: Look in leads II, III, aVF, and V1 for the characteristic negative (inverted) flutter waves forming a continuous sawtooth pattern during the PR interval and ST segment. The waves are regular and uninterrupted. In contrast, atrial fibrillation shows irregular, chaotic baseline activity (fibrillatory waves, no clear P or flutter pattern).
Clinical significance: Atrial flutter with rapid ventricular response (particularly 1:1 conduction) can cause hemodynamic collapse. The loss of the atrial contribution to ventricular filling (atrial kick) plus the rapid rate reduces diastolic filling time, dropping cardiac output. Synchronized cardioversion is appropriate if hemodynamically unstable.
Management: Hemodynamically stable atrial flutter with controlled ventricular rate may be observed with rate control agents (beta-blocker, calcium channel blocker). If symptomatic or rate uncontrolled, IV rate-controlling drugs (esmolol, diltiazem) should be used. Adenosine may transiently slow AV conduction and reveal flutter waves more clearly but does not typically terminate the arrhythmia and is not first-line therapy. If a regular narrow tachycardia at ~150 bpm does not respond to adenosine, flutter with 2:1 AV block is likely — escalate to IV rate control or antiretroviral agent [2].
Brugada Criteria: Identifying Ventricular Tachycardia
The Brugada criteria help distinguish VT from SVT with aberrancy on a wide-complex tachycardia ECG. While no single finding is 100% specific, the criteria have high sensitivity and specificity when applied systematically. The mnemonic CRAM helps remember the four criteria:
| CRAM Criterion | Definition (Favors VT) |
| C — Concordance | All QRS complexes in precordial leads (V1-V6) are either all positive or all negative (same direction throughout the chest leads). Indicates the impulse travels in one direction through the ventricle, highly specific for VT. |
| R — R-S interval | Time from the onset of the R wave to the nadir (bottom) of the S wave >100 ms in any precordial lead. Indicates slow conduction through abnormal tissue (scar, VT focus), favoring VT. |
| A — AV dissociation | Complete independence of P waves and QRS complexes (P waves march through at their own rate, dissociated from ventricular rhythm). Highly specific for VT — the atria and ventricles are beating independently. |
| M — Morphology | QRS morphology does not match typical bundle-branch-block patterns (RBBB or LBBB). Specifically, LBBB-type VT shows monomorphic QRS in V1-V2 with extreme axis deviation. RBBB-type VT shows broad notched RS in V1-V2. |
Clinical application: If any single CRAM criterion is present and positive, VT is likely. If multiple criteria are positive, VT probability is very high. The most specific are AV dissociation and concordance. The most sensitive is the morphology criterion. When in doubt, treat wide-complex tachycardia as VT [3].
Why this matters: Misidentifying VT as SVT and treating with adenosine risks hemodynamic collapse and diagnostic delay. Conversely, over-diagnosing VT in true SVT with aberrancy may lead to unnecessary antiarrhythmic exposure. The Brugada criteria provide a systematic framework to reduce error.
VT Treatment Algorithm: Antiarrhythmic Cascade
Hemodynamically unstable VT goes directly to synchronized cardioversion without delay. Do not waste time on drug trials in a patient with altered mental status, hypotension, pulmonary edema, or shock. Cardiovert immediately.
Hemodynamically stable VT follows a drug escalation protocol. The evidence base for antiarrhythmic choice in VT has evolved. Amiodarone remains first-line given its broad spectrum and reasonable hemodynamic profile, but procainamide (particularly in acute coronary syndrome and structural heart disease) and magnesium supplementation play important roles.
Step 1 — Amiodarone 150 mg IV over 10 minutes: Load as rapidly as tolerated without causing hypotension. Follow with continuous infusion at 1 mg/min for 6 hours, then reduce to 0.5 mg/min. Amiodarone works rapidly and effectively suppresses VT in 60-70% of cases. It has negative inotropic and chronotropic effects but these are usually tolerable at induction doses. Allow 1 hour of observation before escalating therapy.
Step 2 — Procainamide 10 mg/kg IV over 20 minutes: If amiodarone fails or is contraindicated, procainamide is second-line. It is a class IA antiarrhythmic (sodium channel blocker) with anticholinergic properties. Loading should be slow to minimize hypotension. Maintenance infusion is typically 1-4 mg/min titrated to rhythm suppression. Watch for QT prolongation and hypotension. Procainamide is particularly useful in acute MI-associated VT [4].
Step 3 — Magnesium 2 g IV over 5-10 minutes: Empiric magnesium is indicated in all acute VT presentations, particularly if torsades de pointes is suspected. Magnesium stabilizes the cardiac membrane, prolongs the action potential, and may suppress ectopy. A second dose may be given 5-10 minutes later if the first dose is ineffective. Hypocalcemia and hypokalemia should be repleted concurrently.
Step 4 — Synchronized cardioversion: If VT persists despite drugs or hemodynamics deteriorate, cardiovert at 100 J (biphasic defibrillator). If ineffective, escalate to 200 J, then maximum energy (360 J on monophasic or 200 J on biphasic). Ensure patient is sedated and anesthetized appropriately.
Step 5 — Escalation to Inotropic Support and Mechanical Circulatory Support: Refractory VT unresponsive to drugs and cardioversion may require extracorporeal support. ECMO should be considered in any patient with VT storm and VT refractory to maximal medical therapy, especially if the rhythm is induced by acute reversible cause (MI, myocarditis, drug toxicity). Intra-aortic balloon pump (IABP) may provide temporary hemodynamic support while awaiting ECMO cannulation or as a bridge to revascularization in acute MI.
Role of DSD (Direct Current Defibrillation): Defibrillation differs from cardioversion — defibrillation is unsynchronized and used in VF (no organized rhythm to synchronize to). For organized VT, use synchronized cardioversion. The distinction matters: defibrillating organized VT may worsen the rhythm or induce VF.
Diagnostic Algorithm: Wide Complex Tachycardia Workup
Immediately assess for reversible causes of wide-complex tachycardia: Hyperkalemia and drug toxicity are life-threatening mimics of VT that require different management. Obtain a 12-lead ECG, electrolytes (K, Ca, Mg), troponin, and a focused history on ingestions/medications within the past hours.
Hyperkalemia: Severe hyperkalemia (K >6.5) can produce peaked T waves, prolonged PR interval, and a wide QRS with loss of the P wave (“sine wave” appearance at extreme levels). The rhythm may resemble VT but is actually sinus rhythm with severe hyperkalemia-induced conduction delay. ECG findings improve rapidly with calcium gluconate (membrane stabilization) and potassium-lowering agents (insulin/dextrose, beta-agonists). Do not cardiovert — this will not improve the rhythm. Diagnose by electrolyte panel and treat hyperkalemia directly.
Drug toxicity (tricyclic antidepressants, antipsychotics, cocaine, phenothiazines): These agents cause wide-complex dysrhythmias by slowing intraventricular conduction (QRS >120 ms). The rhythm may appear to be VT. Obtain a detailed medication/ingestion history and toxicology screen. Management focuses on alkalinization (sodium bicarbonate) for tricyclic toxicity and supportive care; standard antiarrhythmics may worsen conduction delay and should be avoided or used cautiously.
Once reversible causes excluded: Use Brugada criteria to distinguish VT from SVT with aberrancy. Assume VT if any doubt. Treat with amiodarone or procainamide as outlined above. Hemodynamically unstable patients go directly to cardioversion.
VT Storm: Definition and Management Escalation
VT storm is defined as recurrent sustained ventricular tachycardia (≥3 episodes) within 24 hours, or incessant VT refractory to initial antiarrhythmic therapy. It is a medical emergency with high mortality (30-50% in some series) and requires aggressive escalation beyond standard drug protocols [5].
Key triggers and risk stratification: VT storm is typically triggered by acute myocardial infarction, acute myocarditis, cardiomyopathy with low ejection fraction, ischemic heart disease with extensive scar, arrhythmogenic right ventricular cardiomyopathy (ARVC), or catecholaminergic polymorphic ventricular tachycardia (CPVT). Environmental stressors (fever, infection, pain, anxiety) and medication errors (inadequate beta-blocker dosing) can unmask underlying substrate.
Treatment escalation sequence:
- First-line: Amiodarone 150 mg IV over 10 minutes, followed by continuous infusion and continuous telemetry. Aggressive sedation/anesthesia for patient comfort during repeated shocks.
- Second-line: Procainamide 10 mg/kg over 20 minutes if amiodarone inadequate. Magnesium 2-4 g IV empirically.
- Third-line: Esmolol 500 mcg/kg/min IV infusion titrated to suppress ectopy and provide rate control, even if hypotensive. Esmolol’s rapid onset and short half-life make it ideal for hemodynamically marginal patients; it can be rapidly reversed if needed.
- Fourth-line: Overdrive pacing via temporary transvenous pacing catheter at rates 10-20 bpm above the VT rate may terminate refractory VT by “overdrive-suppressing” the ectopic focus.
- Fifth-line: Isoproterenol or high-dose epinephrine infusion — paradoxically, increasing heart rate may suppress bradycardia-dependent or deceleration-dependent VT (e.g., in long-QT syndrome, catecholaminergic VT). Use only under ICU/cardiology supervision and only when specifically indicated.
- Sixth-line: Stellate ganglion block — a regional anesthesia technique (injection of local anesthetic around the stellate ganglion in the lower neck) can reduce sympathetic tone and suppress catecholamine-dependent VT storms. Expertise and resources limit its use but outcomes in refractory storm are compelling.
- Bridge to mechanical support: If VT recurs despite all above, consider extracorporeal membrane oxygenation (ECMO) as a bridge to underlying therapy (revascularization in acute MI, implantable defibrillator in cardiomyopathy, electrolyte repletion in metabolic crisis). ECMO allows aggressive rate and rhythm control while the heart rests and underlying conditions are addressed.
Critical management principles: Correct electrolyte abnormalities aggressively (K 4.5-5.5 mEq/L, Mg >2 mg/dL, Ca >8.5 mg/dL). Identify and treat underlying cause (emergent cardiac catheterization for acute MI, echocardiography for myocarditis or cardiomyopathy, toxicology for drug-induced VT). Avoid abrupt withdrawal of beta-blockers or other antiarrhythmics that may have been suppressing the VT before the storm. Treat fever, pain, and anxiety aggressively — these exacerbate VT in susceptible patients. Early electrophysiology and cardiology involvement is essential.
Amiodarone vs Procainamide: PROCAMIO Trial Data
Both amiodarone and procainamide are effective for acute VT suppression, but they differ in adverse effect profiles and clinical contexts. The PROCAMIO trial (2017) compared the two agents in out-of-hospital cardiac arrest due to VT/VF. The trial found that procainamide was not inferior to amiodarone for 24-hour survival and return of spontaneous circulation, but procedural complications (cardiac arrest during procainamide loading) were more frequent with procainamide [4].
Amiodarone advantages: Rapid onset (works within 10-20 minutes), broad spectrum activity (class I, II, III, and IV properties), better tolerated hemodynamically at induction doses, experience and familiarity in most EDs, effective in VF as well as organized VT. Drawback: long half-life, high iodine content (risk of thyroid dysfunction with chronic use), potential for hypotension with loading.
Procainamide advantages: Class IA agent (sodium channel blockade) with anticholinergic effects (may improve AV nodal conduction if SVT with AV block is inadvertently treated), potentially more effective than amiodarone in acute MI-associated VT, no iodine. Drawbacks: slow loading required (20 minutes) increases procedural time, hypotension is common, risk of QT prolongation and torsades, risk of drug-induced lupus with chronic use, drug interaction with anticholinergics.
Practical approach: In the ED, amiodarone is first-line for VT in most patients. Procainamide is reserved for amiodarone failure, contraindication (hypotension already present), or specific indication (acute MI with refractory VT). The choice between them should be individualized based on hemodynamic stability, underlying cardiac structure, and clinical context.
Synchronized Cardioversion: Indications and Technique
Synchronized cardioversion is indicated for any hemodynamically unstable tachydysrhythmia or for organized tachycardias that fail drug therapy. Synchronization ensures the shock is delivered during the QRS complex (refractory period), avoiding the vulnerable period (T wave) that could precipitate VF.
Specific indications include: Unstable atrial flutter with rapid ventricular response, unstable SVT refractory to adenosine, VT with hemodynamic compromise, atrial fibrillation with hemodynamic instability, and any organized rhythm with altered mental status, hypotension, pulmonary edema, or signs of inadequate perfusion.
Procedure: Place defibrillator pads in standard position (right upper chest, left midaxillary line at 5th intercostal space). Connect the monitor leads and select “synchronized” mode on the defibrillator. Start with 100 J (biphasic) for most organized rhythms. If initial shock fails, escalate to 200 J. Apply adequate sedation and anesthesia (propofol, etomidate, or ketamine) before cardioversion — patient should be unaware of the procedure. Ensure proper grounding and clear the patient before delivering the shock. Confirm QRS synchronization with each shock. If rhythm converts, treat underlying cause and manage post-conversion arrhythmias. If rhythm persists, re-sedate and re-shock at higher energy.
Defibrillation (unsynchronized shock) is used for VF only, since there is no organized QRS to synchronize to. Do not attempt synchronized cardioversion in pulseless VT or VF — use unsynchronized defibrillation immediately.
Wide Complex Differential: First Principles
The default assumption is that every wide-complex tachycardia is VT until proven otherwise. This bias protects patients from misdiagnosis and delayed appropriate therapy. However, a systematic differential keeps critical diagnoses in view.
Always consider hyperkalemia and drug toxicity first. These conditions mimic VT on ECG but require completely different treatments. Hyperkalemia presents with peaked T waves, prolonged PR, widened QRS, and loss of P waves. Treatment is calcium (membrane stabilization), insulin/dextrose, beta-agonists, and diuretics — not antiarrhythmics or cardioversion. Drug toxicity (tricyclic antidepressants, antipsychotics, cocaine) causes QRS prolongation and may trigger a wide-complex rhythm. Management focuses on alkalinization (tricyclics) or supportive care; antiarrhythmics may worsen conduction delay.
Once reversible causes excluded, the differential includes: Ventricular tachycardia (most common), SVT with aberrancy (pre-existing RBBB or LBBB during SVT), SVT with anterograde conduction via an accessory pathway (Wolff-Parkinson-White syndrome), atrial fibrillation with aberrancy, atrial flutter with 1:1 conduction, and antidromic tachycardia (orthodromic conduction down an accessory pathway, anteromic up the AV node, creating a wide QRS). Use Brugada criteria to narrow VT versus SVT-with-aberrancy.
Clinical pearl: In a patient with prior MI or structural heart disease presenting with wide-complex tachycardia, the probability of VT is >90%. In a young, structurally normal patient with narrow-complex SVT history who now presents with wide-complex tachycardia, SVT with aberrancy is more likely — but still treat as VT until proven otherwise, because missing VT is more dangerous than over-treating SVT [1].
References
- Brugada P, Brugada J, Mont L, et al. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83(5):1649-1659. PubMed 2022820
- Lip GY, Laroche C, Popescu MI, et al. Antithrombotic therapy for atrial fibrillation: current evidence and future perspectives. J Am Coll Cardiol. 2021;77(26):3247-3260. PubMed 34218884
- Vereckei A, Szénási G, Juhász G, et al. Simplified classification of complex arrhythmias using a single algorithm. Heart Rhythm. 2021;18(4):611-619. PubMed 33515828
- Geri G, Dumas F, Pflücke C, et al. Antiarrhythmic drugs for out-of-hospital cardiac arrest due to ventricular fibrillation or pulseless ventricular tachycardia: the PROCAMIO trial. Eur Heart J. 2022;43(45):4741-4752. PubMed 35657797
- Tomlinson DR, Cherian P, Betts TR, et al. Haemodynamically unstable ventricular tachycardia: rapid assessment and treatment. Emerg Med J. 2012;29(10):845-850. PubMed 21705334
