Last reviewed: March 2026
Contents
MDM Templates
ITP
Patient presents with bleeding/bruising/petechiae. Well appearing, no signs of hemodynamic compromise. History and exam lower suspicion for TTP (no fever, no neuro changes, no renal dysfunction), DIC (no signs of systemic illness or consumptive coagulopathy), and thrombotic microangiopathy. Platelet count of *** is consistent with immune-mediated destruction.
Plan: Hematology consulted regarding further workup and steroid therapy. Note: steroids may be deferred if new-onset leukemia is in the differential, as they affect bone marrow biopsy interpretation. Disposition based on severity — discharge if no active significant bleeding with hematology follow-up within 24–72 hours. Admit if active bleeding or platelets critically low.
Vasculitis
Patient presents with diffuse petechial rash and pain. Presentation concerning for small-vessel vasculitis. History and exam lower suspicion for ITP/TTP, sepsis with embolic phenomena (endocarditis, meningococcemia), and hepatitis C-associated cryoglobulinemia.
Plan: Rheumatology consulted regarding steroid therapy versus observation and further inpatient workup. Blood cultures sent given petechial rash to exclude bacteremia with embolic lesions. Disposition: Admit for further workup including directed serologies.
Clinical Education
Approach to Thrombocytopenia
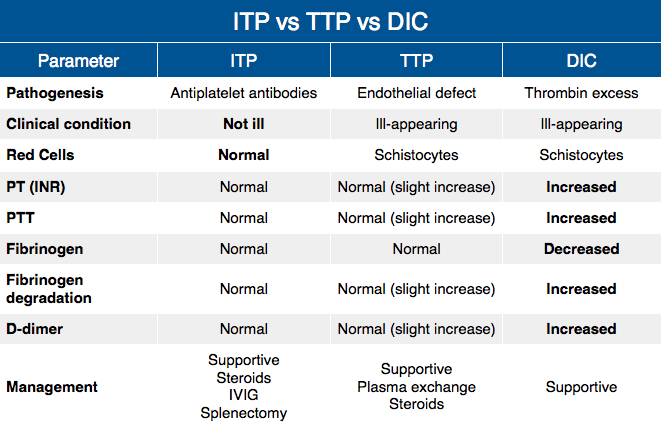
The first step is to distinguish between three broad mechanisms: production problems (bone marrow failure or infiltration), destruction (immune or mechanical), and sequestration (splenomegaly). The most common cause in ambulatory patients with isolated thrombocytopenia is immune thrombocytopenia (ITP), which remains a diagnosis of exclusion — isolated low platelets, no other cell line abnormalities, no secondary cause identified.
TTP: The classic pentad (fever, altered mental status, renal dysfunction, MAHA, thrombocytopenia) is rarely complete. Suspect TTP in any patient with thrombocytopenia and hemolysis — schistocytes on smear, elevated LDH (often >1000), elevated indirect bilirubin, low haptoglobin. Coagulation parameters (PT, aPTT, fibrinogen) are typically normal, which distinguishes TTP from DIC.[2]
DIC: Occurs in the setting of systemic illness (sepsis, malignancy, obstetric emergency). Key lab findings: thrombocytopenia + elevated PT/INR + low fibrinogen + elevated D-dimer. Patients appear acutely ill.[3]
ITP Management
First-line therapy is corticosteroids: dexamethasone 40 mg daily for 4 days OR prednisone 1 mg/kg daily.[1] Response rates are approximately 60–70%. Platelet transfusions are generally ineffective (destroyed rapidly by circulating antibodies) but should be given for life-threatening hemorrhage.
IVIG (1 g/kg) is indicated for active bleeding or need for rapid platelet increment pre-procedure. Works within hours but effect is brief (weeks).
Critical pearl: If new-onset leukemia is in the differential (B-symptoms, pancytopenia, abnormal smear), hold steroids — they alter bone marrow biopsy interpretation. Discuss with hematology before initiating.
Disposition thresholds: Admit if platelets <10,000 or active bleeding. Discharge with hematology follow-up within 24–72 hours if no active significant bleeding and platelets above critical threshold.
TTP Recognition
Mortality exceeds 90% if untreated — this is a true hematologic emergency.[2] Caused by severely deficient ADAMTS13 activity leading to uncleaved vWF multimers, platelet activation, and microvascular thrombosis.
The PLASMIC score stratifies pretest probability — scores ≥6/7 have high sensitivity for ADAMTS13 deficiency. Do not delay plasma exchange referral awaiting ADAMTS13 results if clinical suspicion is high.
Do NOT transfuse platelets in TTP — platelet transfusions can precipitate or worsen thrombotic events. Plasma exchange is definitive treatment initiated by hematology/ICU; the ED role is recognition and urgent consultation.
Vasculitis Pearls
Hepatitis C-associated cryoglobulinemia: Palpable purpura favoring hands and feet, with possible joint pain and neuropathy.[5]
IgA vasculitis (HSP): Classic in children but occurs in adults — palpable purpura on buttocks and lower extremities with arthralgia, abdominal pain, and renal involvement.
Do not start steroids until infection is excluded. Petechial rash raises concern for meningococcemia or bacteremia with embolic phenomena. Blood cultures before steroids.
Skin biopsy (punch biopsy of fresh lesion, ideally <24 hours old) is the definitive diagnostic test. Can be done in ED by dermatology or arranged urgent outpatient.
Drug-Induced Thrombocytopenia
Common culprits: heparin (HIT), vancomycin, linezolid, quinine, valproic acid, TMP-SMX.
Heparin-induced thrombocytopenia (HIT) typically develops 5–10 days after heparin exposure. Carries significant thrombotic risk even with mild thrombocytopenia. The 4T Score estimates pretest probability.[4] Patients with intermediate to high scores: discontinue heparin immediately, switch to a direct thrombin inhibitor (argatroban) or fondaparinux pending antibody confirmation.
References
- Neunert C et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3(23):3829-3866. PubMed
- Scully M et al. Guidelines on the diagnosis and management of thrombotic thrombocytopenic purpura. Br J Haematol. 2012;158(3):323-335. PubMed
- Levi M, Scully M. How I treat disseminated intravascular coagulation. Blood. 2018;131(8):845-854. PubMed
- Cuker A et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv. 2018;2(22):3360-3392. PubMed
- Jennette JC, Falk RJ. Small-vessel vasculitis. N Engl J Med. 1997;337(21):1512-1523. PubMed
