Last reviewed: March 2026
Contents
MDM Templates
Blast Exposure — Observation and Discharge
Patient presents after proximity to an explosion. Airway is patent and protected. Hemodynamically stable. Tympanic membranes are intact bilaterally. Vision grossly normal without evidence of globe rupture or hyphema on exam. CXR without pulmonary infiltrates or pneumothorax. ECG without ischemic changes or arrhythmia.
After over 4 hours of observation, patient has no new concerning symptoms. Cardiopulmonary exam is stable, vital signs are reassuring, and abdomen is benign.
Plan: Observation period completed.
Disposition: Discharge with return precautions for new hearing changes, shortness of breath, chest pain, abdominal pain, or visual changes. Follow up with PCP within 48 hours.
Blast Injury — Significant / Admit
Patient presents after proximity to explosion with injuries consistent with blast exposure. Primary, secondary, and tertiary blast injuries assessed.
Trauma surgery consulted regarding extent of injuries and disposition. Patient managed as a trauma activation.
Plan: Resuscitation per ATLS protocol. Imaging and labs as dictated by clinical findings. Serial reassessment for evolving blast injury pathology.
Disposition: Admit for continued monitoring and management.
Clinical Education
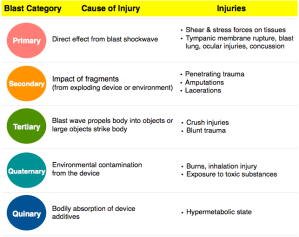
Blast Injury Classification
| Category | Mechanism | Injuries |
| Primary | Overpressure wave (unique to blast) | TM rupture, blast lung, bowel perforation, globe rupture |
| Secondary | Flying debris / shrapnel | Penetrating injuries, fractures, lacerations |
| Tertiary | Body thrown by blast wind | Blunt trauma, traumatic amputation, crush injuries |
| Quaternary | Everything else | Burns, inhalation injury, CO poisoning, chemical exposure |
Tympanic Membrane Rupture
TM rupture is the most common primary blast injury and serves as a marker of blast exposure. However, intact TMs do NOT rule out other primary blast injuries — you can have blast lung with intact eardrums. Examine both TMs in every blast patient. Treatment is conservative: ofloxacin otic drops may speed recovery. ENT follow-up for audiometry and possible tympanoplasty.[1]
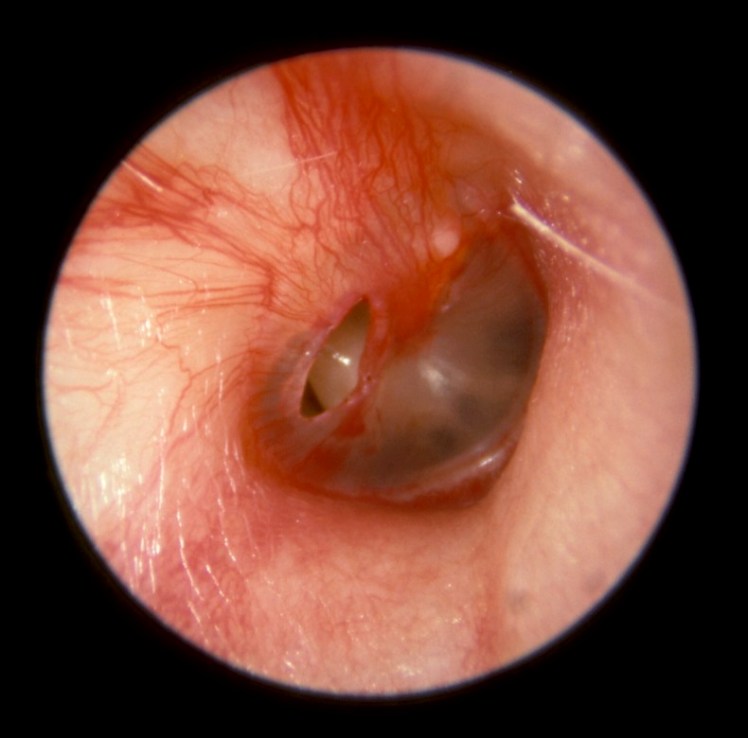
Tympanic membrane rupture from blast
Blast Lung
Blast lung presents like a pulmonary contusion — bilateral infiltrates, hypoxia, hemoptysis. It’s caused by the overpressure wave disrupting alveolar-capillary interfaces. CXR findings may be delayed. Patients with blast lung who require intubation need baroprotective ventilator settings: low PEEP, tidal volumes of 5–7 mL/kg IBW, oxygen saturation goal >90%, permissive hypercapnia (unless concomitant TBI). Consider ECMO for refractory cases.[2]
Deadly Complications
Arterial gas embolism occurs when the blast wave creates bronchovenous fistulae, allowing air to enter the pulmonary veins and travel to the cerebral or coronary circulation. Presents as stroke-like symptoms or sudden cardiovascular collapse in a blast patient. Treatment: 100% FiO2, left lateral decubitus with Trendelenburg positioning, and hyperbaric oxygen when clinically stable.[3]
Bowel perforation can present in a delayed fashion — the overpressure wave causes serosal tears that progress to perforation hours later. Maintain a high index of suspicion for abdominal injuries in blast patients, even with an initially benign exam.
CO poisoning: Indoor blasts produce carbon monoxide. Get a carboxyhemoglobin level on all indoor blast patients. Venous COHb correlates well with arterial levels — VBG is sufficient.
Burns and Lacerations
Don’t fluid-overload the burn patient who may also have blast lung. Aggressive fluid resuscitation for burns can worsen pulmonary edema in the setting of blast-damaged alveolar-capillary membranes. Resuscitate judiciously and monitor closely for respiratory decompensation.[2]
Lacerations from blasts should be considered contaminated. Empiric antibiotics are reasonable — gram-positive coverage (cephalexin, clindamycin) for extremity wounds, broad-spectrum coverage for abdominal/central wounds.
Pregnant Patients
The fetus is relatively protected by amniotic fluid from the blast overpressure wave, but the placenta can shear from the uterine wall due to its different tissue density. Admit all pregnant blast patients for observation, fetal monitoring, and ultrasound. Consider MRI/CT for better placental imaging if concern for abruption.[4]
References
- DePalma RG et al. Blast injuries. N Engl J Med. 2005;352(13):1335-1342. PubMed
- Wolf SJ et al. Blast injuries. Lancet. 2009;374(9687):405-415. PubMed
- Leibovici D et al. Blast injuries: bus versus open-air bombings — a comparative study of injuries in survivors of open-air versus confined-space explosions. J Trauma. 1996;41(6):1030-1035. PubMed
- Peleg K et al. Blast injury and pregnancy. Injury. 2008;39(10):1093-1095. PubMed
