Last reviewed: March 2026
Contents
MDM Templates
Hordeolum (Stye)
Patient presents with a tender, localized swelling of the eyelid consistent with a hordeolum. Vision is unaffected. No limitation of extraocular movements. No proptosis or chemosis. Well appearing.
History and exam reassure against orbital cellulitis, preseptal cellulitis, chalazion with secondary infection, and lacrimal gland pathology.
Plan: Warm compresses for 15 minutes QID. NSAIDs for discomfort. No topical antibiotics indicated — little evidence they alter the course.
Disposition: Discharge. Ophthalmology referral if not improving within 1–2 weeks. Return precautions for spreading redness, fever, vision changes, or EOM limitation.
Chalazion
Patient presents with a painless or mildly tender nodule in the eyelid without surrounding cellulitis. No vision changes. No limitation of EOM. This is consistent with a chalazion (chronic granulomatous inflammation of a meibomian gland).
History and exam reassure against preseptal cellulitis, orbital process, and lacrimal tumor.
Plan: Warm compresses for 15 minutes QID and gentle lid massage. No antibiotics indicated.
Disposition: Discharge. Most resolve spontaneously over weeks to months. Ophthalmology referral if persistent beyond 4–6 weeks for possible incision and curettage.
Preseptal (Periorbital) Cellulitis
Patient presents with eyelid swelling, erythema, and tenderness. Vision is preserved. Extraocular movements are full without pain. No proptosis. No chemosis. No afferent pupillary defect.
Presentation consistent with preseptal cellulitis. The key clinical distinction is the absence of orbital signs (proptosis, ophthalmoplegia, vision loss, chemosis) that would suggest orbital cellulitis.
Plan: Oral antibiotics — amoxicillin-clavulanate 875/125 mg PO BID for 10 days (covers skin flora including MSSA and streptococci). Add TMP-SMX or doxycycline if MRSA concern.
Disposition: Discharge with PCP follow-up in 24–48 hours. Return precautions for worsening swelling, fever, vision changes, pain with eye movement, or inability to move the eye.
Orbital Cellulitis Concern
Patient presents with eyelid swelling and erythema with concerning features: ***. The presence of proptosis, painful or limited extraocular movements, chemosis, and/or vision changes raises concern for orbital cellulitis — an infection posterior to the orbital septum.
Given orbital signs, I have considered orbital cellulitis, subperiosteal abscess, cavernous sinus thrombosis, and orbital compartment syndrome. This is most commonly a complication of sinusitis.
Plan: CT orbits with IV contrast. IV antibiotics initiated — vancomycin + ampicillin-sulbactam (or ceftriaxone + metronidazole). Blood cultures obtained.
Ophthalmology and ENT consulted regarding imaging findings, abscess drainage candidacy, and disposition.
Disposition: Admit for IV antibiotics and serial ophthalmic exams.
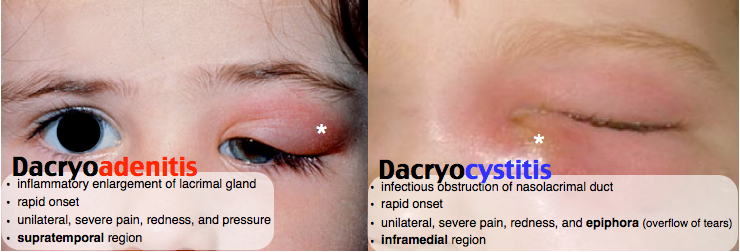
Dacryocystitis
Patient presents with pain, swelling, and erythema over the medial canthus at the nasolacrimal sac (inferomedial to the medial canthal tendon). Tearing (epiphora) and purulent discharge expressible from the punctum on palpation.
Presentation consistent with acute dacryocystitis. History and exam reassure against preseptal cellulitis, orbital cellulitis, and lacrimal gland tumor.
Plan: Oral antibiotics — amoxicillin-clavulanate 875/125 mg PO BID for 10 days. Warm compresses QID. Gentle lacrimal sac massage.
If abscess present: I&D may be indicated. Ophthalmology consultation for consideration of dacryocystorhinostomy (DCR) as outpatient.
Disposition: Discharge with ophthalmology follow-up in 1–2 weeks. Return precautions for fever, worsening swelling, or vision changes.
Dacryoadenitis
Patient presents with unilateral supratemporal orbital pain and swelling localized to the lacrimal gland region (superolateral orbit). No vision changes. EOM intact.
Presentation consistent with dacryoadenitis. History and exam reassure against orbital cellulitis, lacrimal tumor, and other causes of lid swelling.
Plan: Warm compresses and NSAIDs. Antibiotics if bacterial infection suspected (amoxicillin-clavulanate).
Chronic or recurrent: ophthalmology referral for evaluation of underlying systemic disease (sarcoidosis, thyroid disease, lymphoma).
Disposition: Discharge with PCP follow-up in 1 week.
Clinical Education
Preseptal vs Orbital Cellulitis
The orbital septum is the clinical and anatomic dividing line. Preseptal cellulitis (anterior to the septum) presents with lid swelling, erythema, and tenderness but preserved vision, full EOM, no proptosis, and no pain with eye movement. Orbital cellulitis (posterior to the septum) adds proptosis, painful/limited EOM, decreased vision, chemosis, and afferent pupillary defect. When in doubt, CT orbits with contrast.[1]
In children age <1 year, CT is indicated earlier — the exam is unreliable because you cannot accurately assess vision, EOM, or proptosis in an infant with a swollen-shut eye. Sinusitis (especially ethmoid) is the most common source for orbital cellulitis in children.[1]
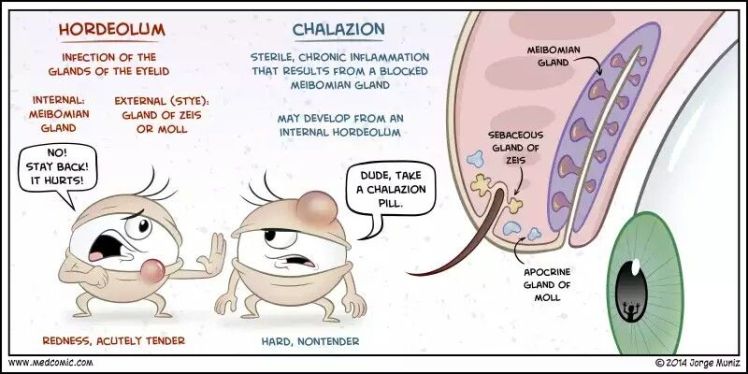
Hordeolum and Chalazion Pearls
Hordeolum (stye) is an acute, tender, infected gland of the eyelid. External hordeola (gland of Zeis or Moll) point at the lid margin. Internal hordeola (meibomian gland) are deeper and may point toward the conjunctival surface. Both are typically caused by S. aureus. Treatment is warm compresses — topical antibiotics have no proven benefit but are commonly prescribed.[2]
Chalazion is a chronic, painless granuloma from an obstructed meibomian gland. Unlike a hordeolum, it is non-infectious. Most resolve with warm compresses over weeks to months. Referral for incision and curettage if persistent. Recurrent or atypical chalazia should prompt consideration of sebaceous cell carcinoma, especially in older patients.[2]
Dacryocystitis and Dacryoadenitis
Location is the key differentiator: dacryocystitis involves the nasolacrimal sac (inferomedial canthus — lower lid area), while dacryoadenitis involves the lacrimal gland (superolateral orbit — upper lid area). Dacryocystitis is much more common and is caused by nasolacrimal duct obstruction leading to stasis and infection. Common in infants (congenital duct stenosis) and older adults.[3]
Chronic dacryoadenitis warrants workup for sarcoidosis, thyroid disease, lymphoma, and other systemic inflammatory conditions. Bilateral lacrimal gland enlargement is a red flag for systemic disease.
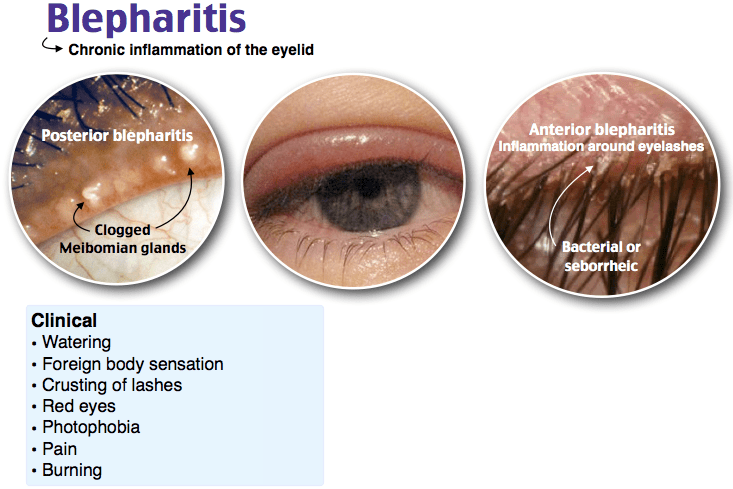
Blepharitis
Blepharitis is chronic inflammation of the eyelid margins — the most common cause of chronic red, irritated eyes. Patients present with crusty, flaky lids, burning, and foreign body sensation. Anterior blepharitis (at the lash line) is often staphylococcal or seborrheic. Posterior blepharitis (meibomian gland dysfunction) produces a thickened, expressible, toothpaste-like secretion from the meibomian glands.[2]
Treatment is lid hygiene: warm compresses for 5–10 minutes followed by gentle lid scrubs with dilute baby shampoo on a cotton swab along the lash line. Makeup avoidance during flares. Refractory cases may benefit from topical azithromycin or oral doxycycline (for meibomian gland dysfunction).
Disposition
Hordeolum, chalazion, blepharitis: discharge with PCP or ophthalmology follow-up PRN. Preseptal cellulitis: discharge on oral antibiotics with close follow-up. Orbital cellulitis: admit for IV antibiotics, imaging, and surgical consultation. Dacryocystitis/dacryoadenitis: discharge on oral antibiotics with ophthalmology follow-up.[1]
References
- Howe L, Jones NS. Guidelines for the management of periorbital cellulitis/abscess. Clin Otolaryngol. 2004;29(6):725-728. PubMed
- Lindsley K et al. Interventions for acute internal hordeolum. Cochrane Database Syst Rev. 2017;1:CD007742. PubMed
- Mills DM et al. The microbiologic spectrum of dacryocystitis: a national study of acute versus chronic infection. Ophthalmic Plast Reconstr Surg. 2007;23(4):302-306. PubMed
